
Premature atrial contractions (PACs) are the most common cause of referral for fetal arrhythmia. They are due to atrial ectopic beats and are seen most commonly in the late second trimester of pregnancy through term and are usually benign. PACs can be either conducted or blocked. PACs are associated with congenital heart disease in up to 2% of cases and can progress to sustained tachycardia in utero or in the first 4 weeks of life in up to 3% of cases. Risk factors for progression of PACs to tachycardia include multiple blocked atrial ectopic beats and complex ectopy inculding bigeminy or trigeminy. Weekly assesment of cardiac rhythm is warranted until delivery (1).
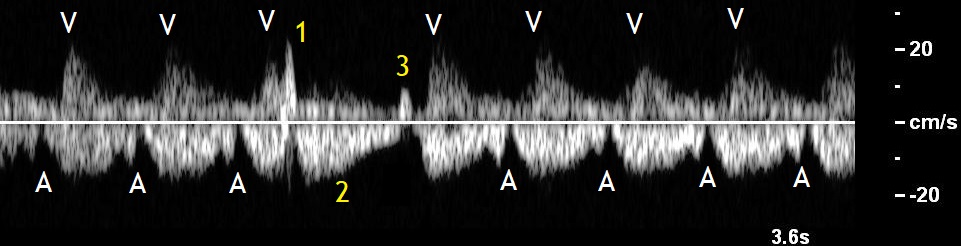
The premature atrial contractions follow a usually normal ventricular contraction and are seen in doppler ultrasound as deep a waves, because they hit on a closed atrioventricular valve. If they are conducted, they are followed by a ventricular contraction which appears to be smaller than usual, because of the smaller stroke volume. The next venous circle will be delayed because of the non-compensatory, post-extrasystolic pause and the ventricular contraction after this circle will be larger than usual. This phenomenon which is called post-extrasystolic potentiating is due to the intact Frank-Starling mechanism (Figure 3) (2).
Most extrasystoles represent an isolated anomaly, not affecting the fetal condition. Their presence should not influence the obstetric care and may require only chocardiographic monitoring (3).



Bibliography
- A practical guide to fetal echocardiography, second edition, Alfred Abuhamad, Rabih Chaoui, 2010.
- Dopplersonographie in Geburtshilfe und Gynäkologie, 3. Auflage, Steiner, Schneider, 2012.
- Respondek M, Wloch A, Kaczmarek P, Borowski D, Wilczynski J, Helwich E. Diagnostic and perinatal management of fetal extrasystole. Pediatr Cardiol.1997 Sep-Oct;18(5):361-6.
