
Indication
- Benign gynecological conditions
- Uterine fibroids causing serious symptoms (with exception of small, singular intracavitary fibroids FIGO I or II).
- High suspicion of adenomyosis uteri interna resistant to endocrine therapy.
- Dysfunctional uterine bleeding resistant to endocrine therapy or endometrial ablation.
- Urogynecological conditions
- Pelvic organ prolapse (in the context of surgical repair of the middle compartment, i.e. laparoscopic sacrocervicopexy).
Technique
- Preoperative antibiotic prophylaxis (single shot, second generation cephalosporine).
- Patient in lithotomy position.
- Desinfection of the abdomen, thighs, vulva and vagina.
- Sterile surgical drapes.
- Urinary catheter.
- Examination under anesthesia.
- Grasp the cervix with bullet forceps and uterine sound. We suggest the use of an atraumatic uterine manipulator. In the setting of lower resources, one may use the bullet forceps and the uterine sound held together as a manipulator. Performing LASH without a manipulator is also possible, however not as safe.
- Change of surgical gloves, start of laparoscopy.

As usual in laparoscopy, inspection of the whole peritoneal cavity should be performed. 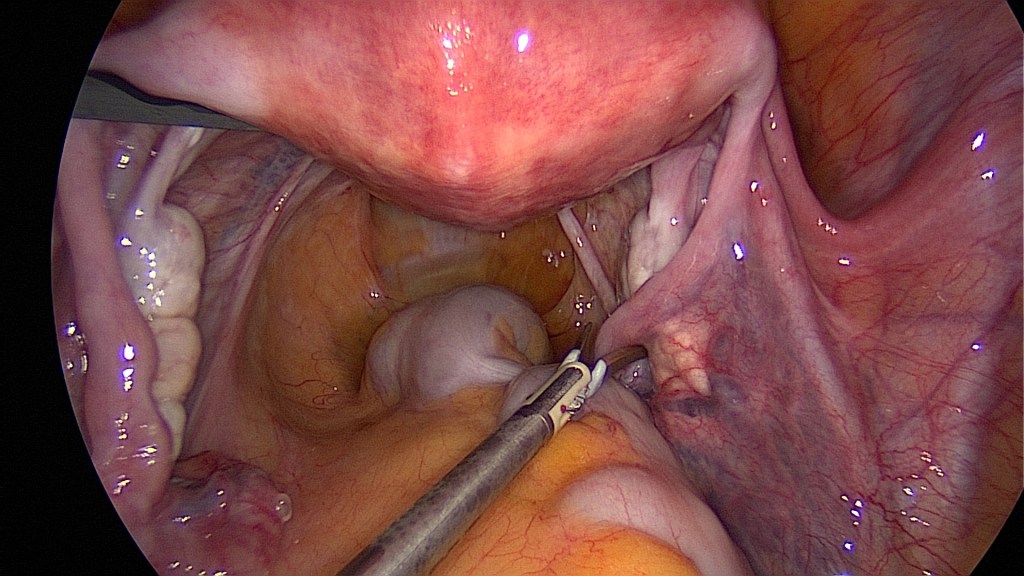
Begin with the oncoprophylactic salpingectomy. 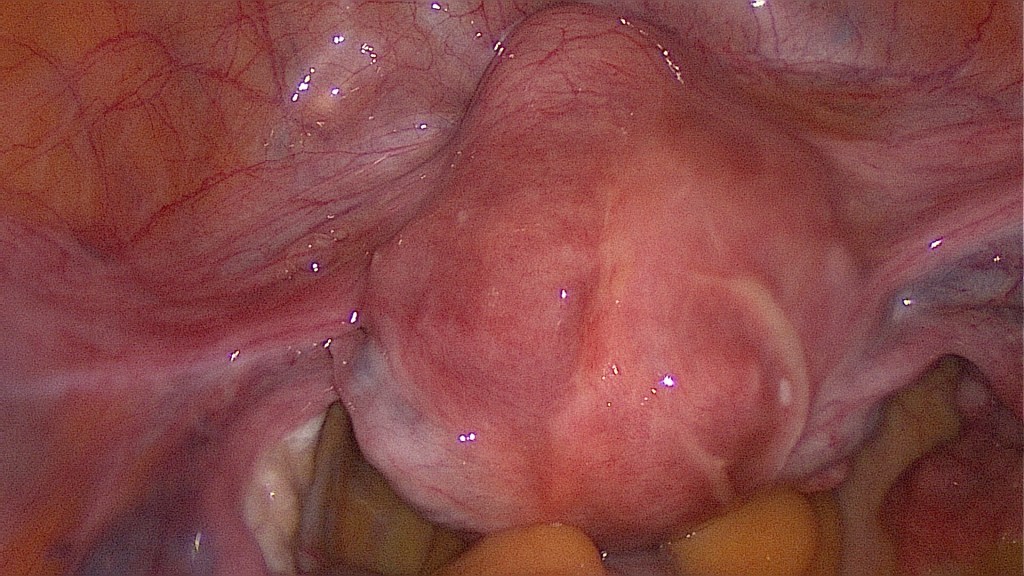
The indication for LASH in this case are the symptomatic uterine fibroids and a co-existing adenomyosis. 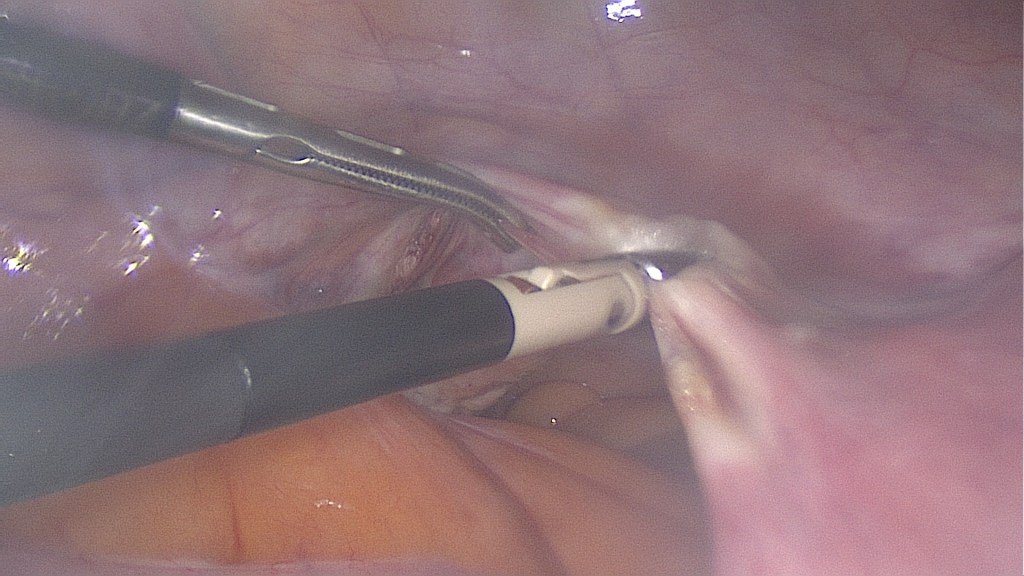
Bipolar coagulation of the left round ligament and the left utero-ovarian ligament. 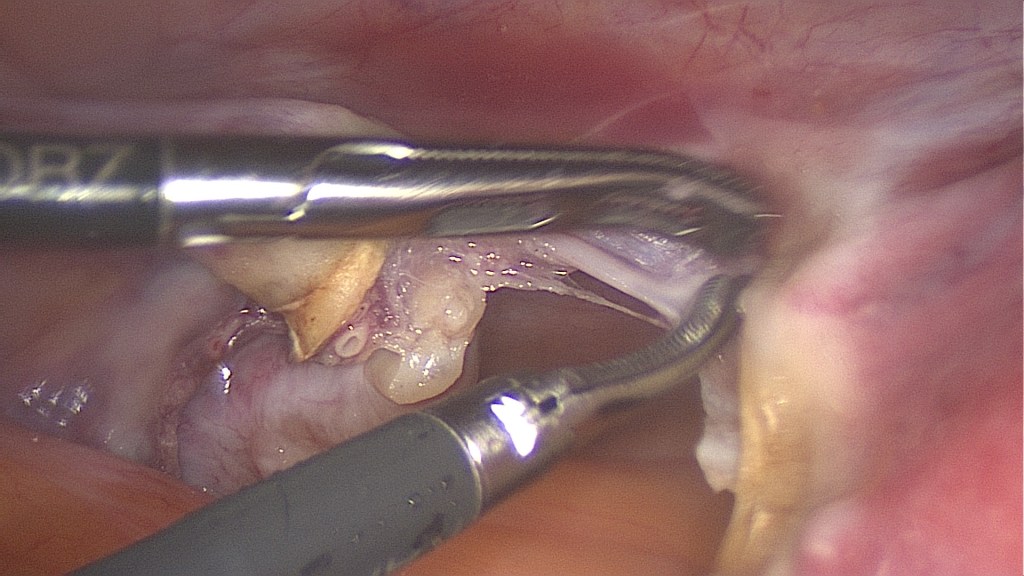
Cutting of these ligaments. 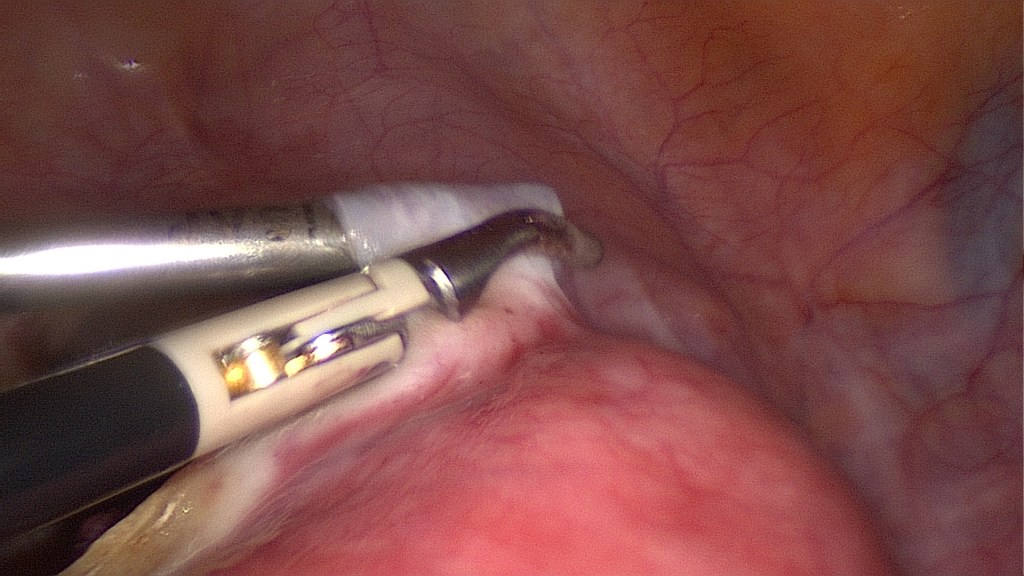
Separation of the bladder peritoneum. 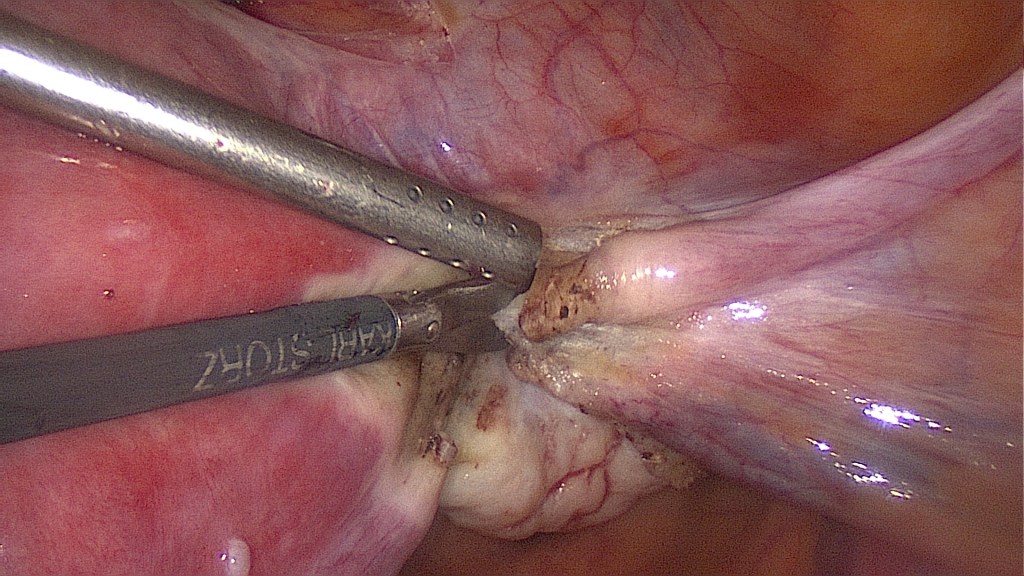
Same procedure on the right side. Here the cutting of the round and utero-ovarian ligaments. 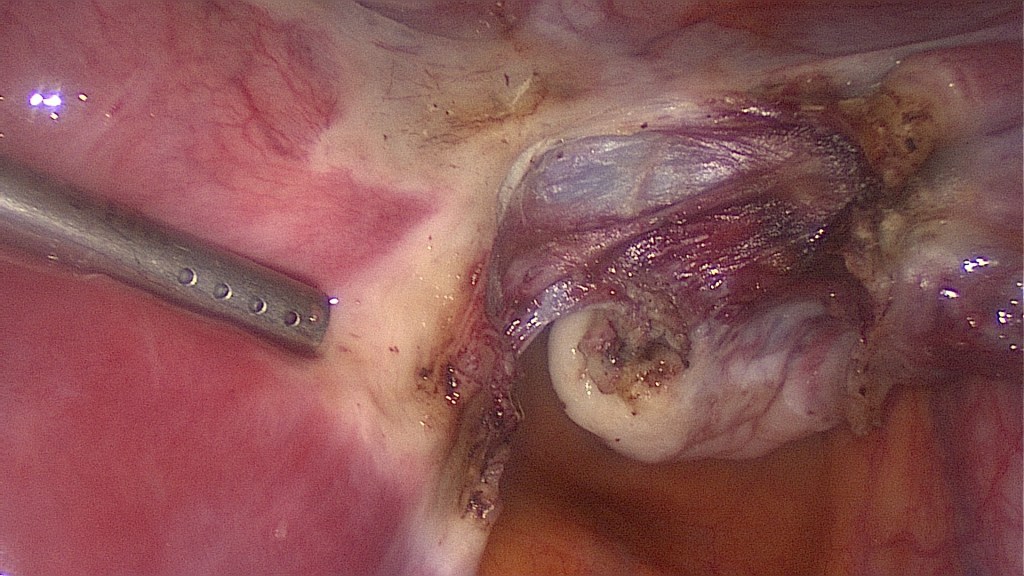
Image after these ligaments have been cut. 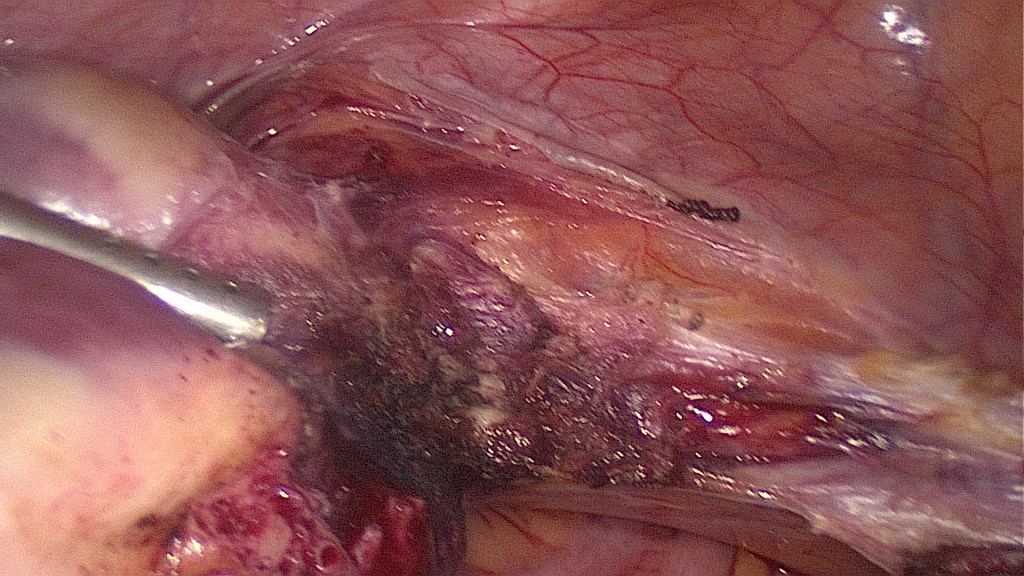
Complete separation of the bladder peritoneum. 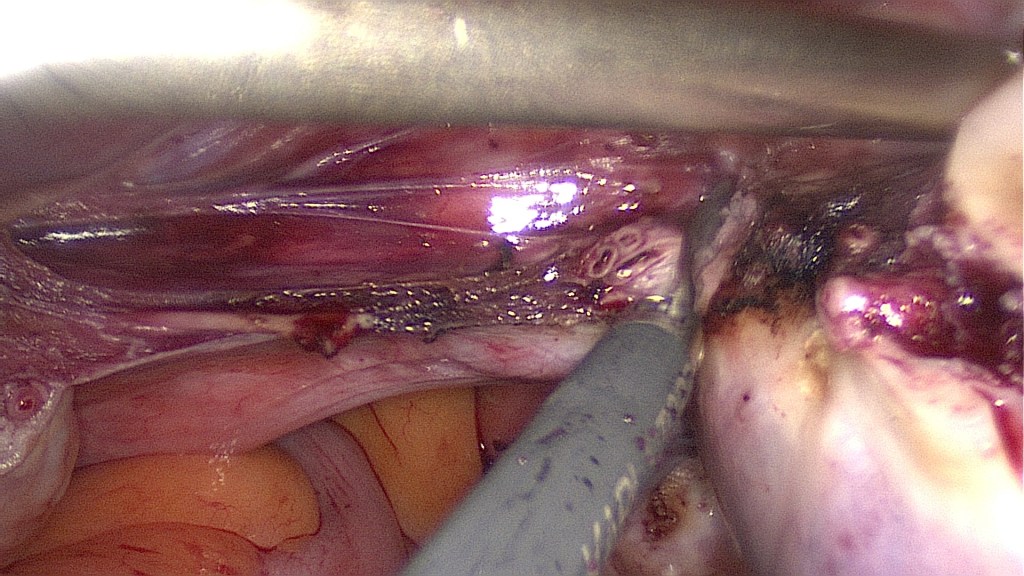
Bipolar coagulation and cutting of the left uterine vessels, first on the left then on the right. 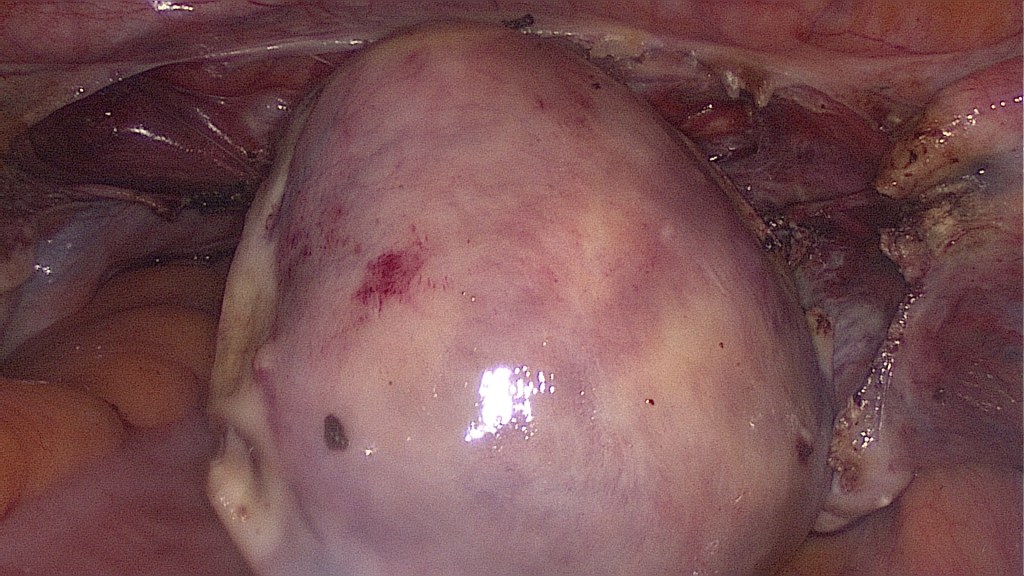
The vessel supply has been taken out and the uterus is getting livid. 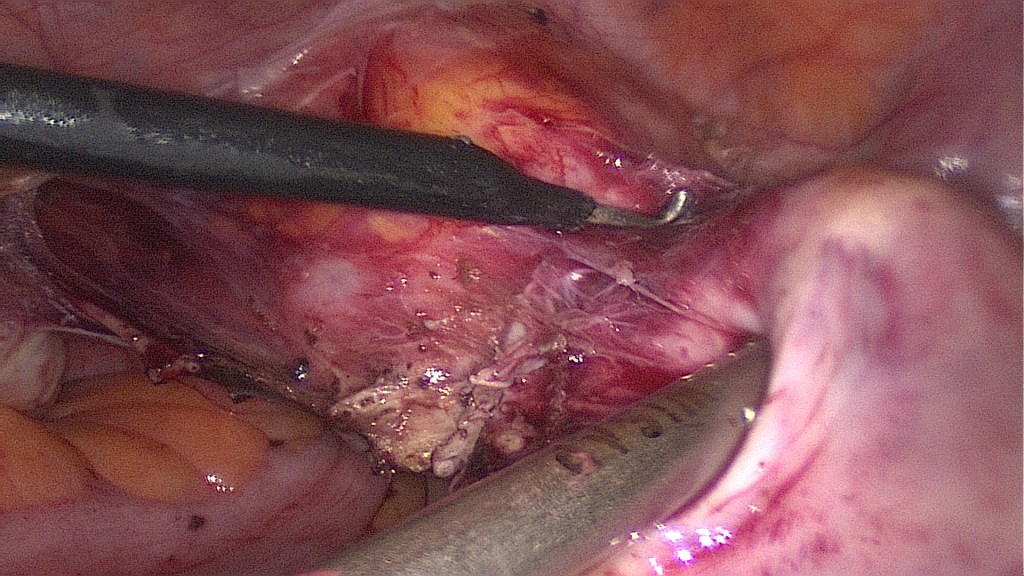
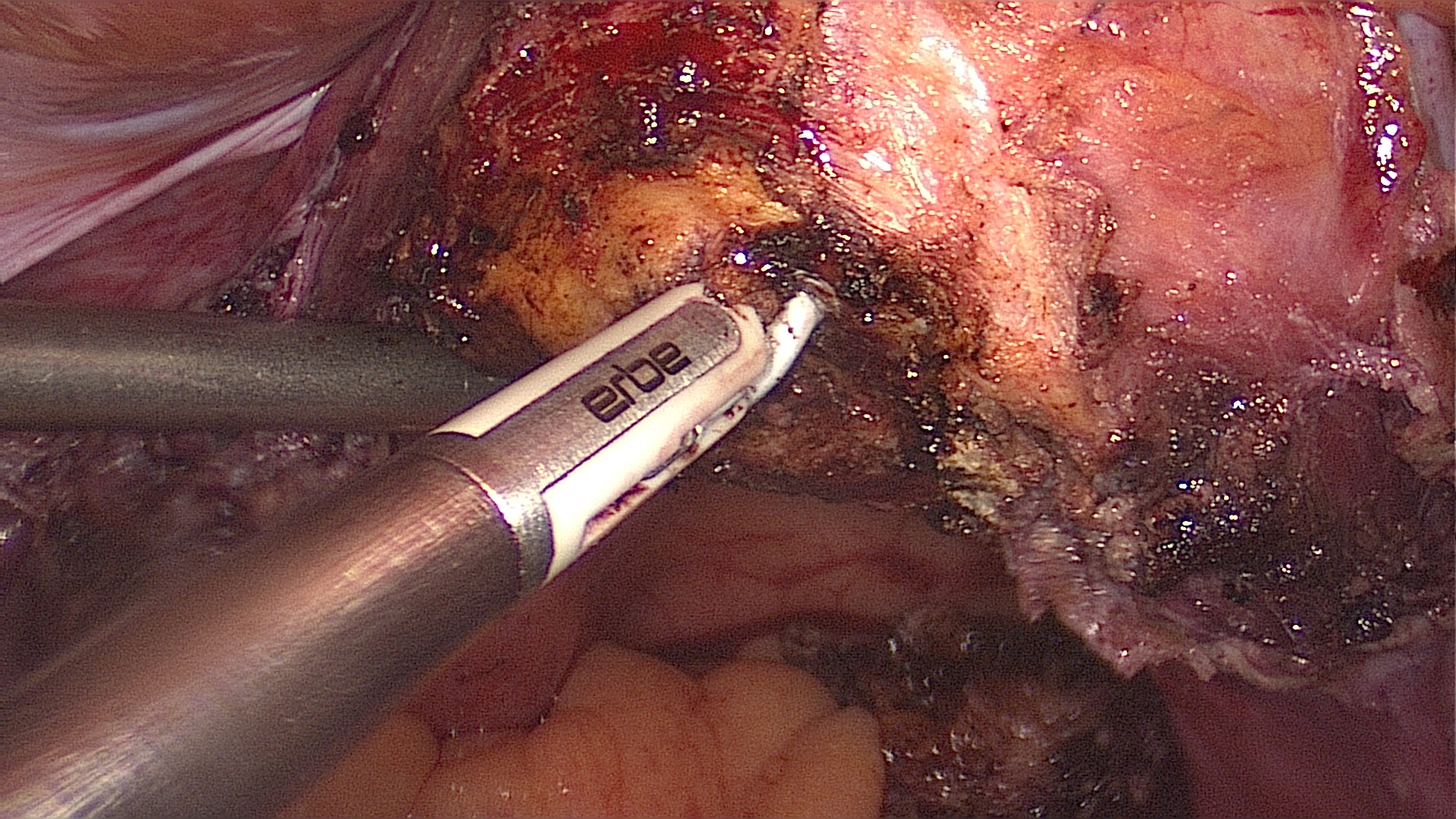
Performing a cut with monopolar cautery on the uterine isthmus. Alternatively a monopolar loop or even the simple scissors may be used. Caution is advised, as this is probably the most dangerous step of the procedure. 
Bipolar coagulation of the cervical canal to minimize cyclic bleeding. 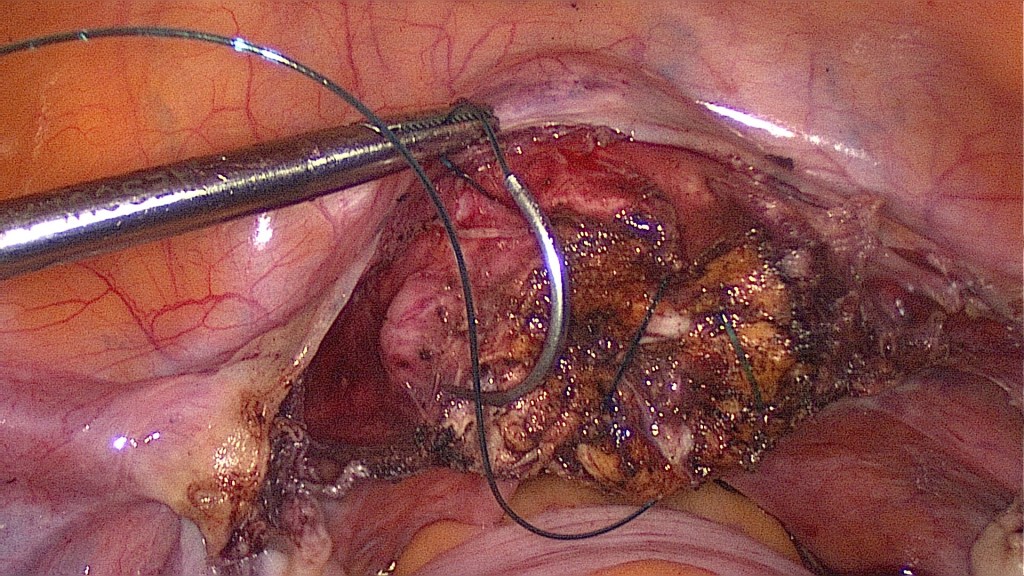
We prefer suturing the internal cervical os with a figure of 8 PDS suture. This helps hemostasis and may prevent ascending infection. 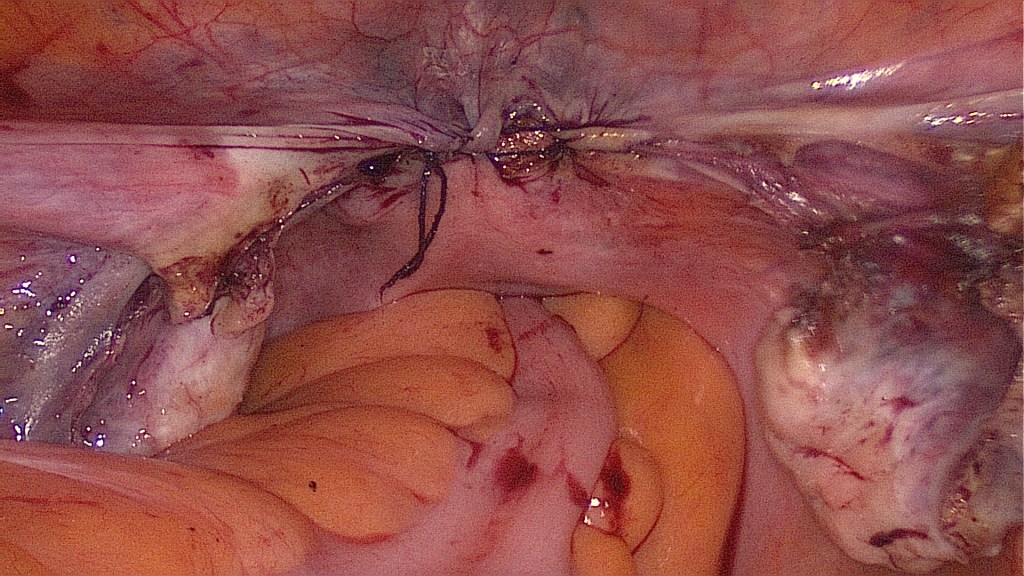
Closure of the peritoneum may allow a more physiologic healing process. 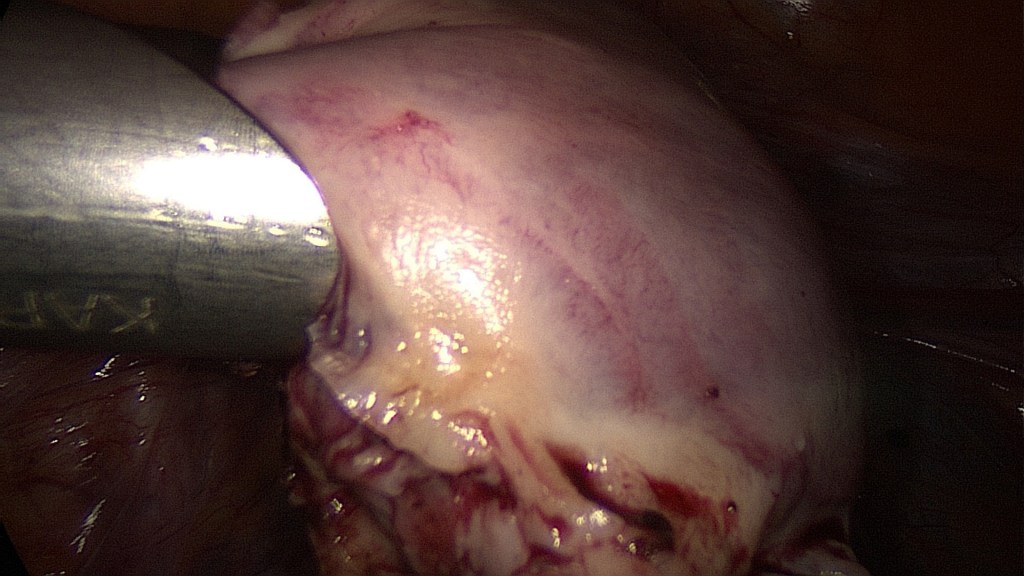
Power morcellation of the uterine body. Thorough, systematic inspection of the abdomen for residual tissue. Removal of the morcellator. 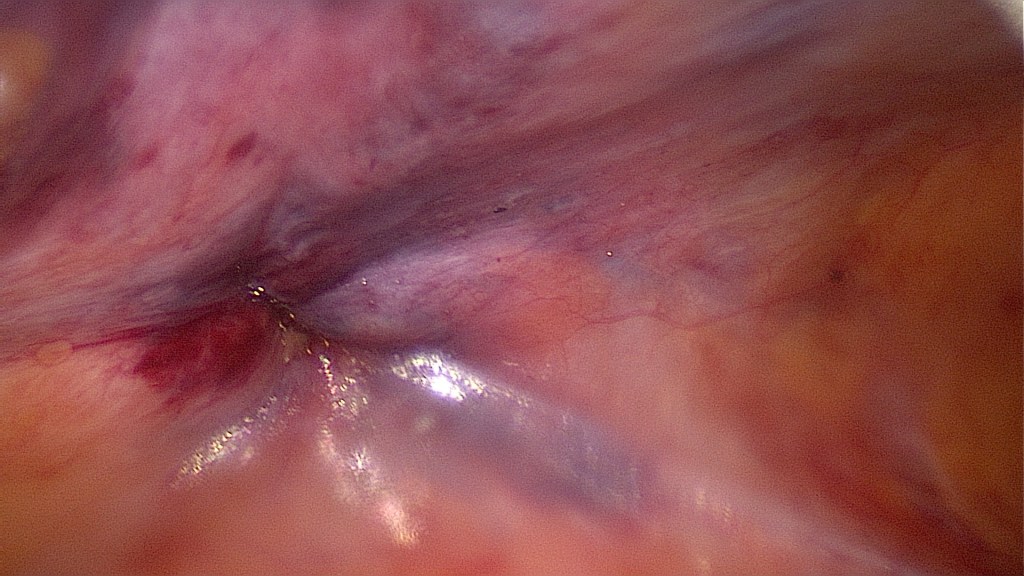
Endoscopic suturing of the fascia along with the parietal peritoneum to prevent postoperative hernia. 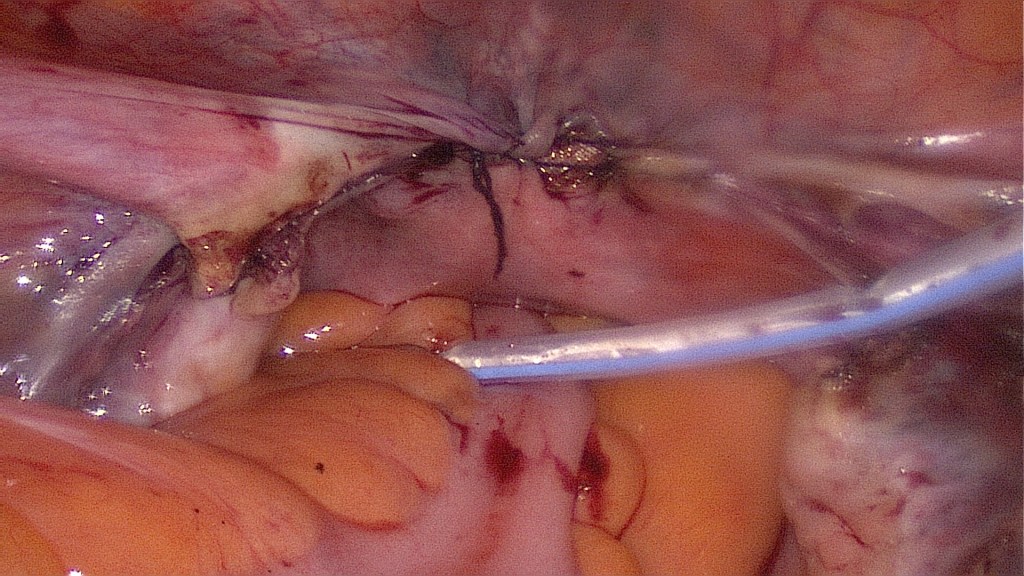
Placement of a drainage.
- Placement of a drainage.
- Removal of instruments and trocars under direct visualization.
- Suturing of the skin.
Contraindications
- Patient not fit for surgery.
- Patient has further plans for bearing children.
Complications
- Injury of nearby organs (ureter, bladder, bowel).
- Bleeding.
- Thromboembolism.
- Infection.
- Dissemination of benign condition or malignancy.
Postoperative Management
- Removal of bladder catheter within the first 24 hours.
- Removal of drainage on 1st postoperative day.
- Routine blood test on 1st postoperative day (Hemoglobin).
- Early patient discharge (usually 3-4 days).
- Venous thromboembolism prophylaxis with low molecular weight heparin for 7 days.
Bibliography
- Neis, K. J., Zubke, W., Fehr, M., Römer, T., Tamussino, K., & Nothacker, M. (2016). Hysterectomy for Benign Uterine Disease. Deutsches Arzteblatt international, 113(14), 242–249. https://doi.org/10.3238/arztebl.2016.0242
- Sandberg, E. M., Hehenkamp, W., Geomini, P. M., Janssen, P. F., Jansen, F. W., & Twijnstra, A. (2017). Laparoscopic hysterectomy for benign indications: clinical practice guideline. Archives of gynecology and obstetrics, 296(3), 597–606. https://doi.org/10.1007/s00404-017-4467-9
- Encke, A., Haas, S., & Kopp, I. (2016). The Prophylaxis of Venous Thromboembolism. Deutsches Arzteblatt international, 113(31-32), 532–538. https://doi.org/10.3238/arztebl.2016.0532
