
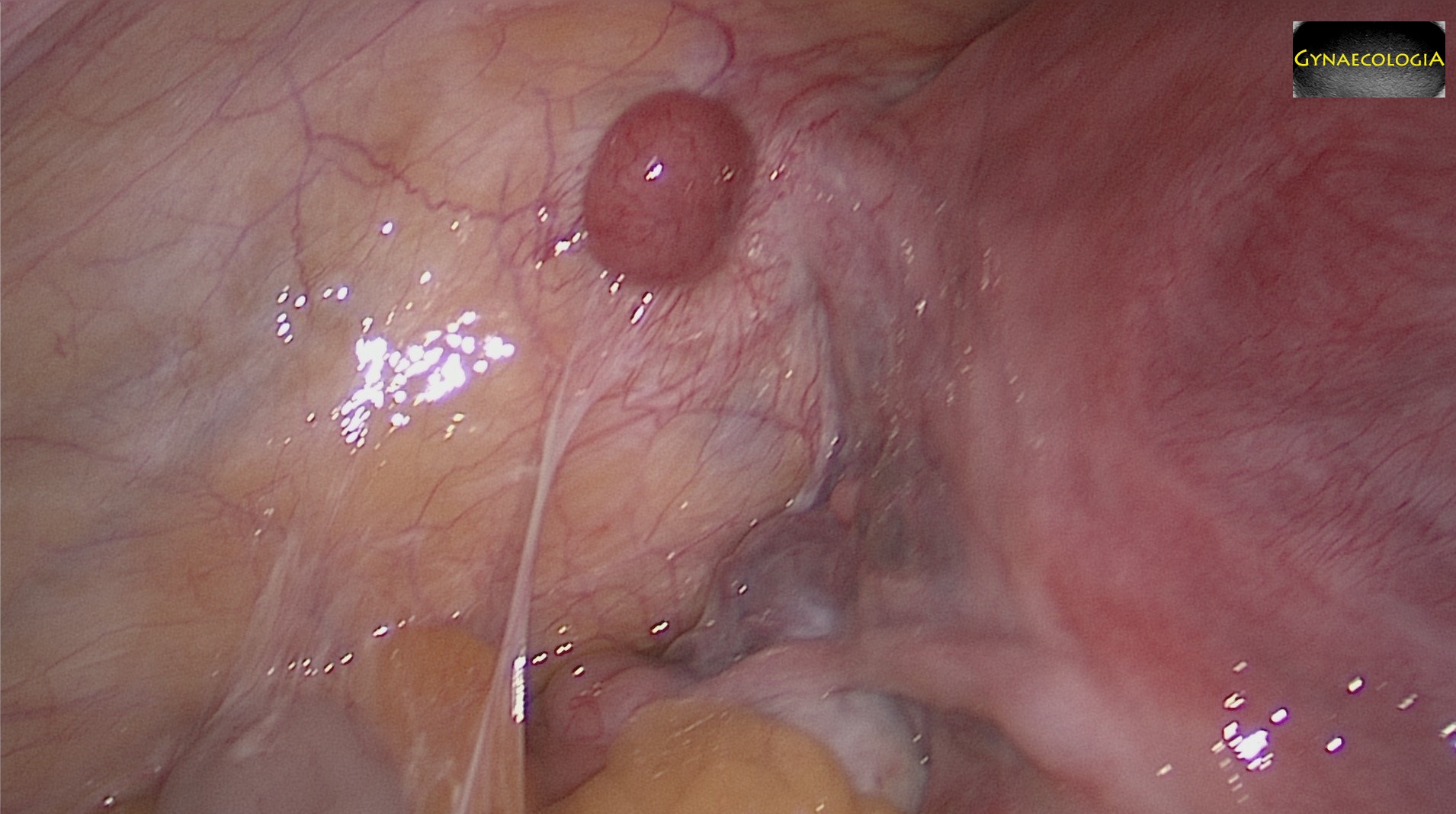
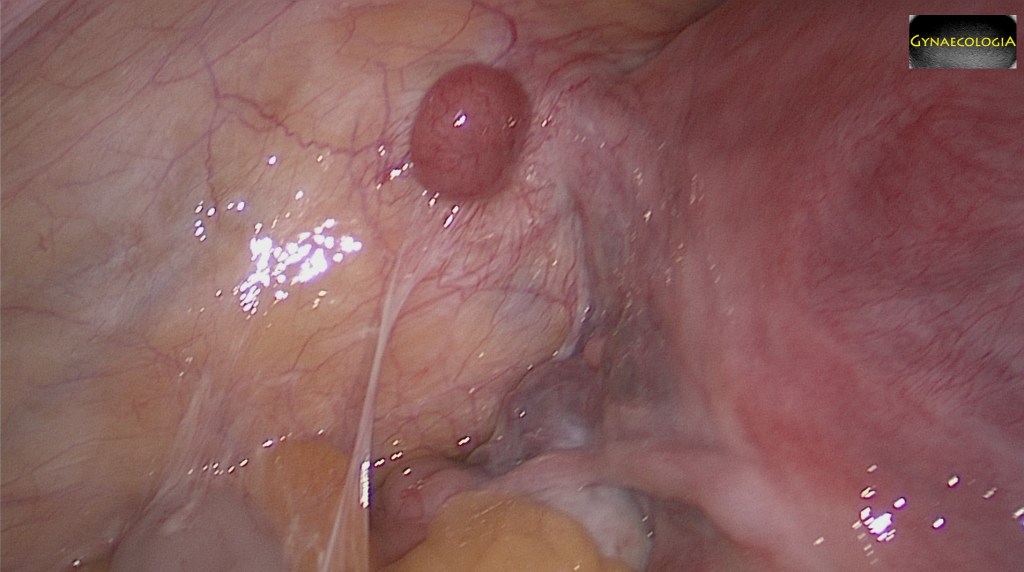
During surgery one may come across solid, round structures that assemble myomas but show no connection to the uterus. In this example, a 50 year old patient comes for a supracervical hysterectomy following three previous laparoscopic myoma enucleations. Of important note, in-bag morcellation was not once used.
Definition/Origins
Parasitic myomas are primarily iatrogenic. They occur mainly after laparoscopic surgery where morcellation without safety precautions took place. These safety precautions refer to the concept of in-bag-morcellation. If left behind, small fragments of myomas may attach themselves onto the peritoneal surface, the omentum, or onto the bowel and promote neoangiogenesis. With newly acquired blood-supply, these may even grow to cause symptoms.
Parasitic myomas are thought to even arise spontaneously after a pedunculated subserosal myoma starts recieving blood supply from another nearby structure and abandons its previous connection to the uterus.
Clinical Image
Most commonly parasitic myomas are incidental findings during surgery for symptomatic uterine myomas. However they may also cause symptoms, most often pain, but even urinary frequency, constipation, dyschezia and other pressure symptoms.
Diagnosis
Diagnosing parasitic myomas can be difficult. The suspicion should arise from the patient’s history. Remember that the most important risk factor for a parasitic myoma is the presence of uterine myomas. The second most important risk factor is previous laparoscopic myoma enucleation where uncontained power morcellation was used. Palpation may sometimes be useful, but ultrasound or even magnetic resonance tomography are excellent modalities in finding bigger parasitic myomas. Sometimes though, these are very small and can only be seen during laparoscopic surgery.
Treatment
The only treatment in case of symptomatic parasitic myomas is adequate surgical excision.
Prevention
Prevention of parasitic myomas comes through exclusive use of in-bag morcellation systems at the time of myomectomy or hysterectomy.
Bibliography
- Kho, K. A., & Nezhat, C. (2009). Parasitic myomas. Obstetrics and gynecology, 114(3), 611–615. https://doi.org/10.1097/AOG.0b013e3181b2b09a
- Boudová, B.arbora, Richtárová, A.déla, Frühauf, F.ilip, Fischerová, D.aniela, & Mára, M.ichal (2022). The role of power morcellation in minimally invasive gynecologic surgery. Role elektrické „power“ morcelace v minimálně invazivní gynekologické operativě. Ceska gynekologie, 87(4), 289–294. https://doi.org/10.48095/cccg2022289
