
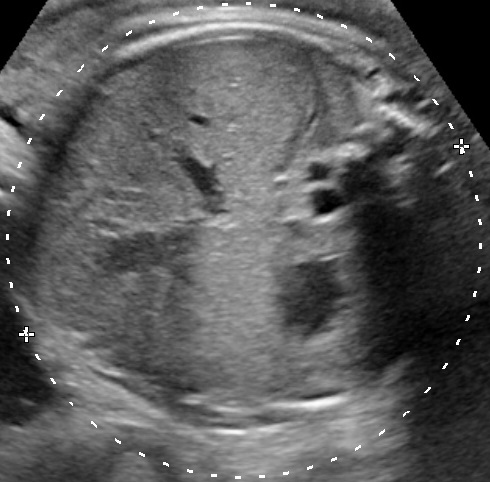
Polyhydramnios is the excessive accumulation of amniotic fluid defined as a single deepest pocket (SDP) of ≥ 8cm or as an amniotic fluid index (AFI) ≥ 24cm. It affects 1–2% of pregnancies. Click here to read more about measuring the amniotic fluid.
Causes
A. Maternal causes of polyhydramnios include:
- Preexisting diabetes mellitus and gestational diabetes (5-26% of the cases),
- kidney failure (increased production in fetal urine secondary to urea-induced osmotic diuresis),
- hypercalcemia,
- treatment with lithium,
- substance abuse.
B. Fetal causes of polyhydramnios can be divided into three categories:
- Increased production of urine
- fetal kidney diseases (polyuric phase by hydronephrosis, Bartter syndrome),
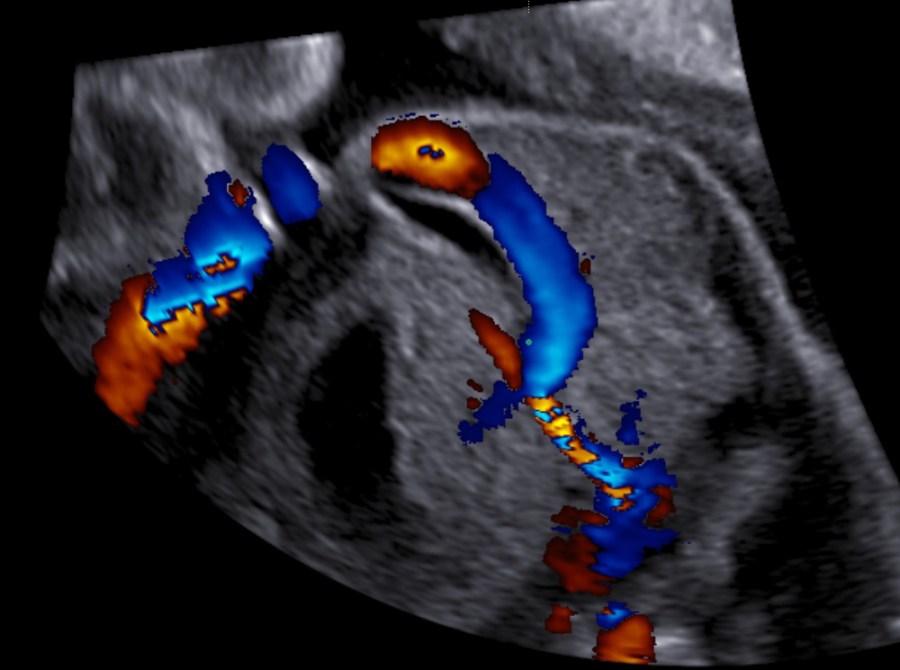
- fetal hypervolemic heart failure (anemia, arrhythmia, tumor, chorangioma, acceptor fetus of the twin-twin transfusion syndrome, pump twin of the TRAP-sequence),
- fetal infections (Parvovirus B19, Toxoplasmosis),
- fetal “overgrowth syndrome” (e.g. Beckwith-Wiedemann syndrome, Sotos syndrome).
- Decreased swallowing
- gastrointestinal/tracheal obstruction (atresia, fistula, diaphragmatic hernia, micrognathia),
- neuromuscular diseases (fetal acinesia deformation sequence, congenital muscle dystrophia, spinal muscle atrophy),
- Prader Willi syndrome.
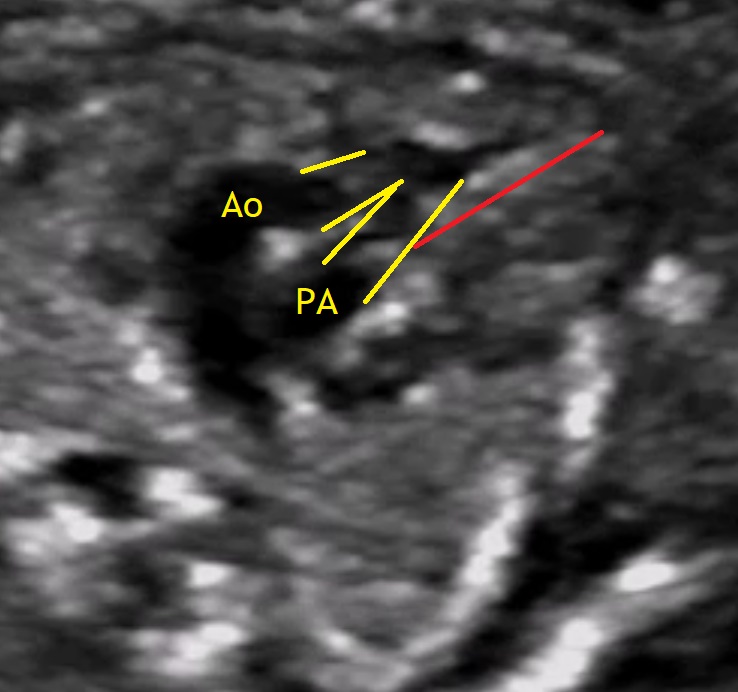
- Other fetal diseases (e.g. Trisomia 18, trisomia 21, anencephaly, skelettal anomalies, spina bifida aperta, congenital chloride diarrhea, omphalocele, structural heart anomalies, lung sequestration, CCAML).
C. Idiopathic
Severe polyhydramnios (AFI > 44) can be associated with fetal malformations in up to 65% of the cases, while milder cases are most commonly idiopathic, or associated with maternal diabetes. This is an important issue while making the differential and during counselling of the mother.
Complications
The more severe the polyhydramnios, the more often are adverse pregnancy outcomes. A small exception appears to be the risk of preterm labor which may be increased but does not correlate to the severity of the polyhydramnios. The following complications are some of the most frequent:
Complications due to over-expansion of the uterus:
- maternal dyspnea,
- preterm labor, premature rupture of membranes,
- abnormal fetal presentation,
- umbilical cord prolapse,
- postpartum hemorrhage (uterine atony).
Diagnosing Polyhydramnios
The gestational week does not influence the diagnosis of polyhydramnios. The size of the uterus could be suggesting of this condition, however the diagnosis should be made during ultrasound examination. There are two common ways to estimate the volume of the amniotic fluid:
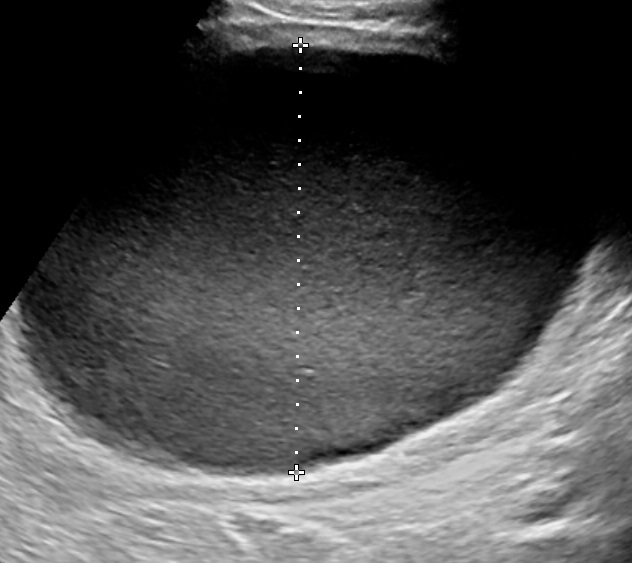
- Single Deepest Pocket (SDP). A vertical measurement in the deepest amniotic fluid pocket. Values below 2 cm indicate oligohydramnios, values over 8 cm indicate polyhydramnios (8-11: mild, 12-15: moderate, > 16: severe). In multiple gestation, a range of 3–8 cm is defined as normal. Another technique is the
- Amniotic Fluid Index (AFI). This is the sum of vertical measurements of all four quadrants (polyhydramnios usually >24).
Work-up (A B C D D)
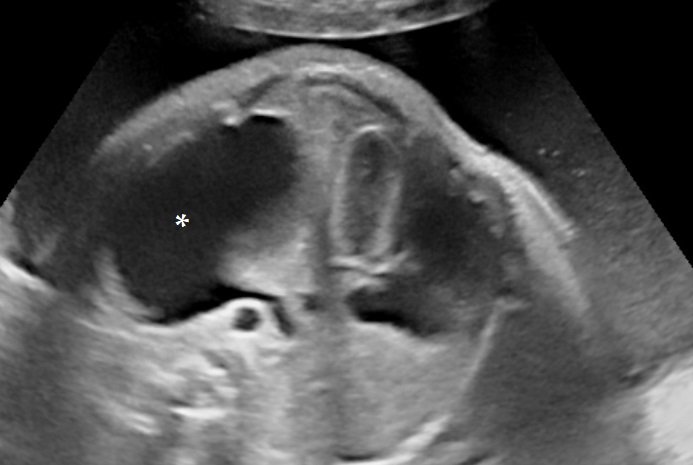
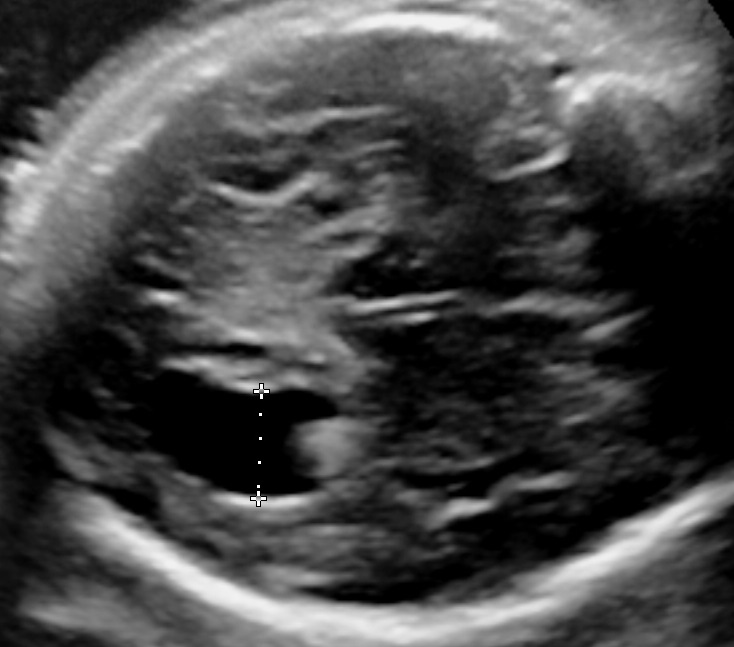
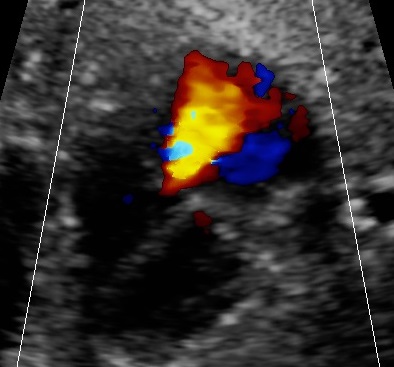
- Anatomy of the fetus and its movements should be examined carefully
- B19 Parvovirus especially but also complete TORCH serologic-screen
- Chromosomes / Karyotyping (and CGH-Array) in cases of severe polyhydramnios where no structural anomalies have been detected
- Diabetes / oral glucose tolerance test (75g)
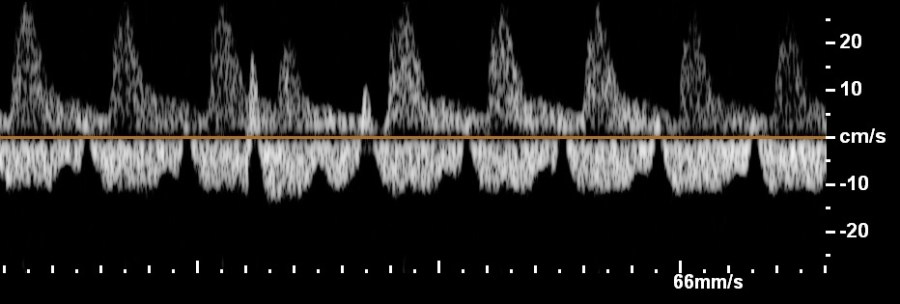
- Doppler velocimetry of the middle cerebral artery to exclude fetal anemia
Idiopathic polyhydramnios which spontaneously resolves bears no risk of congenital anomalies. Still macrosomia remains an important concern.
Treatment
Causal therapy should be attempted. Gestational diabetes should be controlled. Fetal anemia can be treated with transfusion and fetal arrhythmia can be handled with antiarrhythmic agents given to the mother. Naturally, some of the causes that have already been mentioned cannot be treated during pregnancy, meaning that some patients could have persisting polyhydramnios.
This condition of persisting polyhydramnios may cause discomfort. Amniodrainage has proven a good way to relieve maternal discomfort. Possible complications include uterine contractions, PROM, chorioamnionitis and, specifically in twins, inadvertent septostomy resulting in iatrogenic monoamniotic twins. Medication like indomethacin has also been used as a means of reduction of the amniotic fluid, especially in cases of prenatally diagnosed Bartter syndrome (2×0.5mg/kg/day).
Read similar articles:




Bibliography
- Pri-Paz, S., Khalek, N., Fuchs, K. M. and Simpson, L. L. (2012), Maximal amniotic fluid index as a prognostic factor in pregnancies complicated by polyhydramnios. Ultrasound Obstet Gynecol, 39: 648–653. doi:10.1002/uog.10093
- Hershkovitz, R., Sheiner, E., Maymon, E., Erez, O. and Mazor, M. (2006), Cervical length assessment in women with idiopathic polyhydramnios. Ultrasound Obstet Gynecol, 28: 775–778. doi:10.1002/uog.3818
- Rochelson, B., Wagner, J. and Shmoys, S. (1992), The clinical significance of resolving polyhydramnios. Ultrasound Obstet Gynecol, 2: 321–324. doi:10.1046/j.1469-0705.1992.02050321.x
- Leung, W. C., Jouannic, J.-M., Hyett, J., Rodeck, C. and Jauniaux, E. (2004), Procedure-related complications of rapid amniodrainage in the treatment of polyhydramnios. Ultrasound Obstet Gynecol, 23: 154–158. doi:10.1002/uog.972
- Fong, B. F. and de Vries, J. I. P. (2003), Obstetric aspects of the Prader–Willi syndrome. Ultrasound Obstet Gynecol, 21: 389–392. doi:10.1002/uog.90
- Panting-Kemp A, Nguyen T, Castro L. Substance abuse and polyhydramnios Am J Obstet Gynecol. 2002 Sep;187(3):602-5.
- Furaz-Czerpak KR, Fernández-Juárez G, Moreno-de la Higuera MÁ, Corchete-Prats E, Puente-García A, Martín-Hernández R., Pregnancy in women on chronic dialysis: a review, Nefrologia. 2012 May 14;32(3):287-94. doi: 10.3265/Nefrologia.pre2012.Jan.11319. Epub 2012 Feb 28.
- “14 Poly- Und Oligohydramnie.” Fetale Therapie, by Christoph Berg, De Gruyter, 2017, pp. 307–312.
- Hamza A, Herr D, Solomayer EF, Meyberg-Solomayer G. Polyhydramnios: Causes, Diagnosis and Therapy. Geburtshilfe und Frauenheilkunde. 2013;73(12):1241-1246. doi:10.1055/s-0033-1360163.
