
When Valsalva* is performed with an empty bladder:
- Significant bladder neck descent, defined as descent of at least 25mm.
- Open retrovesical angle.
- Reduced urethral sphincter volume.
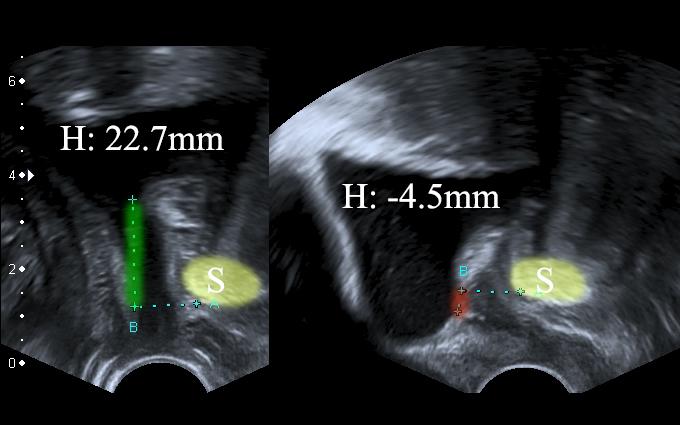
Significant bladder neck descent (ΔH: 27.2mm). Left: patient is relaxed. Right: patient performs Valsalva. 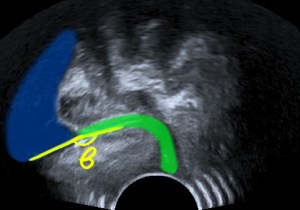
Open retrovesical angle (β). Green: urethra. Blue: bladder. 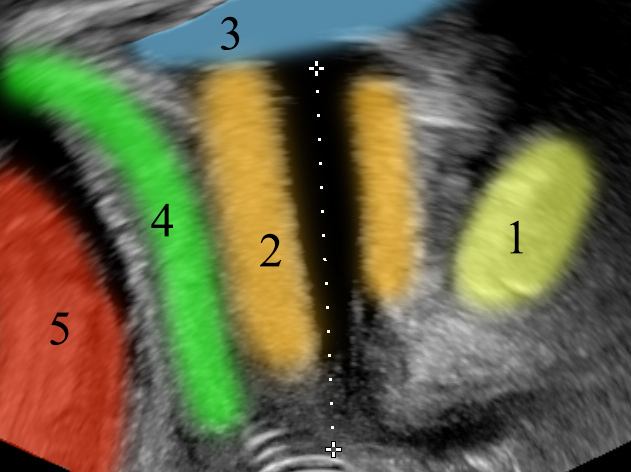
Normal urethra anatomy. 1: symphysis pubis, 2: urethral sphincter, 3: bladder, 4: vagina, 5: rectum.
Do not forget:
It is mid-urethral mobility, not mobility of the bladder neck, which is most important for continence.
When Valsalva* is performed with a full bladder:
- Urine leakage in b-mode or even with color doppler when the bladder is filled.
*Optimal Valsalva is considered when its duration is at least 6 seconds.
Bibliography
- Dietz H. P. (2011). Pelvic floor ultrasound in incontinence: what’s in it for the surgeon?. International urogynecology journal, 22(9), 1085–1097. https://doi.org/10.1007/s00192-011-1402-7
- Naranjo-Ortiz, C., Shek, K. L., Martin, A. J., & Dietz, H. P. (2016). What is normal bladder neck anatomy?. International urogynecology journal, 27(6), 945–950. https://doi.org/10.1007/s00192-015-2916-1
- Dietz H. P. (2019). Ultrasound in the assessment of pelvic organ prolapse. Best practice & research. Clinical obstetrics & gynaecology, 54, 12–30. https://doi.org/10.1016/j.bpobgyn.2018.06.006
- Orejuela, F. J., Shek, K. L., & Dietz, H. P. (2012). The time factor in the assessment of prolapse and levator ballooning. International urogynecology journal, 23(2), 175–178. https://doi.org/10.1007/s00192-011-1533-x

1 Comment