

The descent of the posterior vaginal wall can be due to:
- True Rectocele (defect of the rectovaginal septum).
- Abnormally distensible – however intact -rectovaginal septum.
- Enterocele.
- Rectal intussusception.
- Deficient perineum giving the impression of a “bulge”.
- A combination of the above.
How to diagnose an enterocele?
An enterocele refers to the caudal displacement of small bowel loops. Τhe enterocele typically appears in the posterior vaginal wall, but not exclusively. Rarely it might also appear in the anterior vaginal wall. In post-hysterectomy patients the enterocele sac descends through the middle, displacing the vaginal cuff caudally. Differentiating the enterocele from a rectocele and other types of prolapse is essential for proper surgical planning.
- Demonstrating peristalsis can be held as pathognomonic for small bowel loops.
- The presence of any intraperitoneal fluid may help outline the apex of the enterocele.
- Small bowel contents (ground-glass echogenicity) are usually not difficult to distinguish from stool in the rectal ampulla.
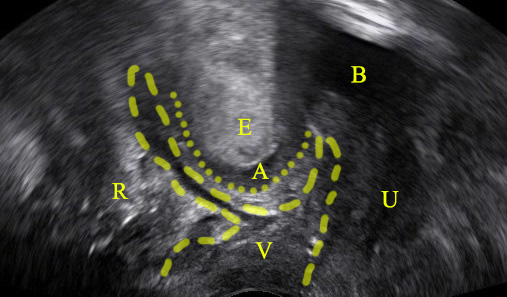
Depicting an enterocele in pelvic floor ultrasound is feasible:

Bibliography
- Dietz HP. Ultrasound in the assessment of pelvic organ prolapse. Best Pract Res Clin Obstet Gynaecol. 2019;54:12-30. doi:10.1016/j.bpobgyn.2018.06.006
