

We present a technique for laparoscopic sacrocervicopexy for treating apical prolapse using three trocars. Concomitant colporrhaphy should be performed at the beginning of the surgery if anterior or posterior prolapse coexist.
Indication
- Uterine prolapse.
Technique
If colporrhaphy is needed, begin with the colporrhaphy.
The laparoscopy begins with the placement of a 10mm umbilical and two accessory 5mm ports on the left (surgeon’s) side. The first of them is placed 3cm lateral of the umbilicus and the second one 2cm medial of the anterior superior iliac spine (ASIS).

Identification of structures. On the left: sigmoid colon. On the right: common iliac artery with bifurcation, right ureter, right fallopian tube. In the middle: promontory. 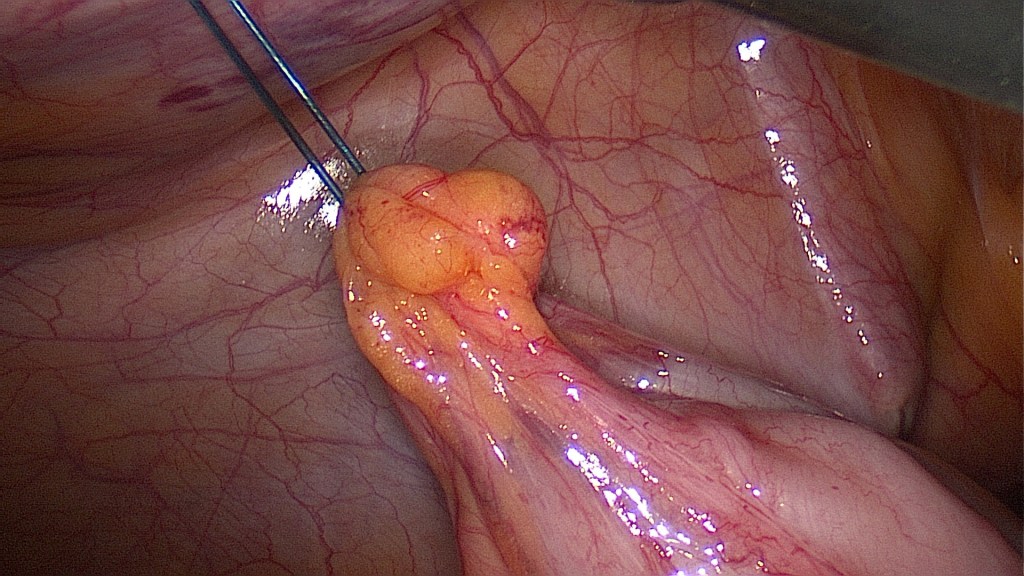
Transient fixation of the sigmoid colon towards the left abdominal wall is a useful, yet non-mandatory step. This facilitates access to the retroperitoneal space along the bed of the mesh and minimizes risk of bowel injury. We prefer a long straight needle which is inserted 2cm above the lower left trocar and passes through at least two epiploic appendices of the sigmoid colon.

Situs after supracervical hysterectomy. 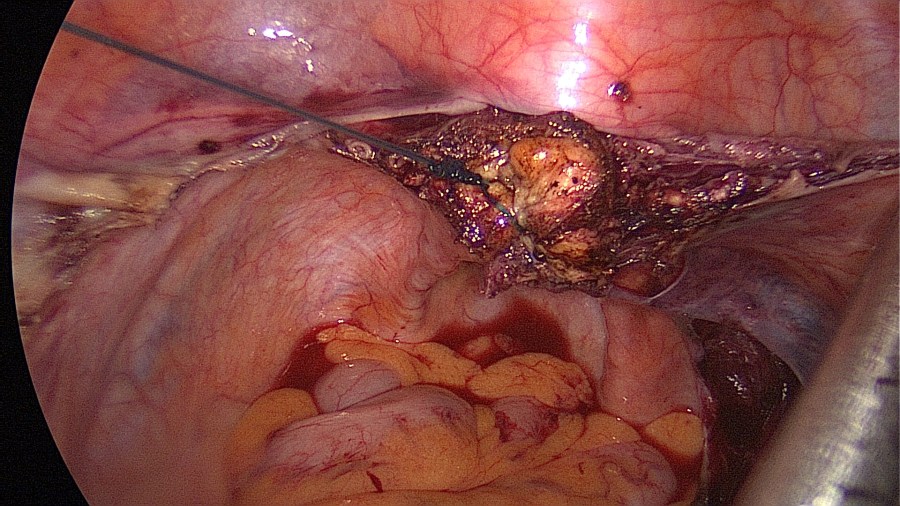
Suturing of the internal cervical os. 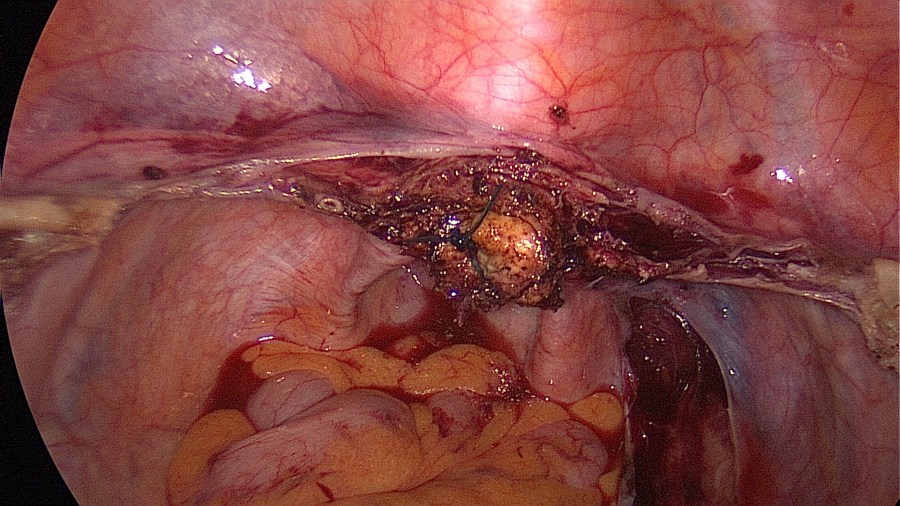
The closed cervical os may prevent ascending infection. Additionally this suture may be used for traction on the cervix to facilitate vision on the dorsal part of the cervix. 
Creation of a retroperitoneal tunnel between the cervix and the promontory. This tunnel helps the peritonization process later since it divides the areas which have to be closed (divide and conquer).
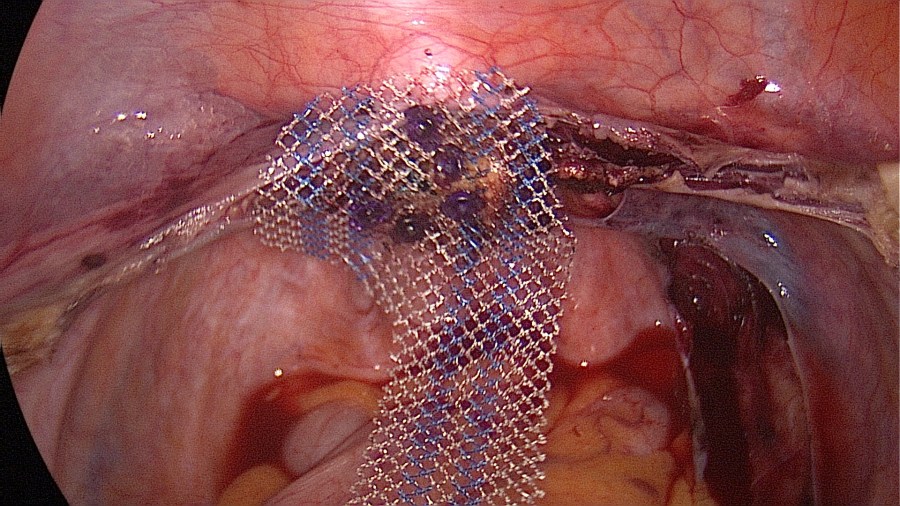
Fixing the mesh facilitates additional suturing. 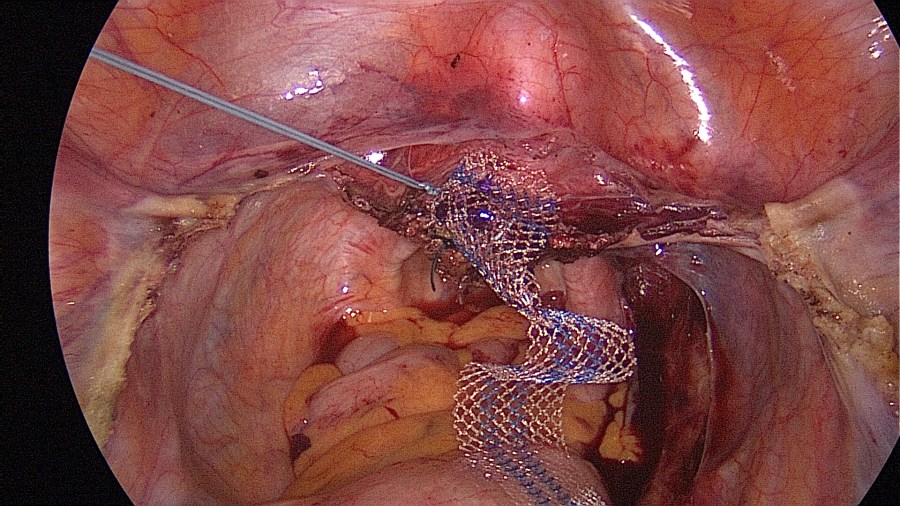
Three non-absorbable sutures are placed and the knots are tied extracorporeally.
The mesh is now passed through the retroperitoneal tunnel. The second assistant elevates the cervix as high as possible, then retracts the cervix 2-3cm.
This motion dictates the correct length of mesh to fixate on the promontory.
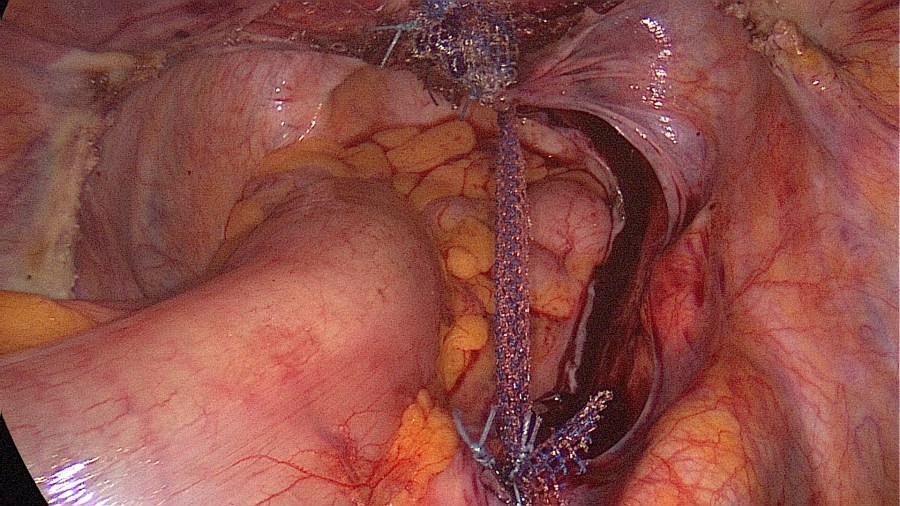
Trim excess mesh. The mesh looks stable. 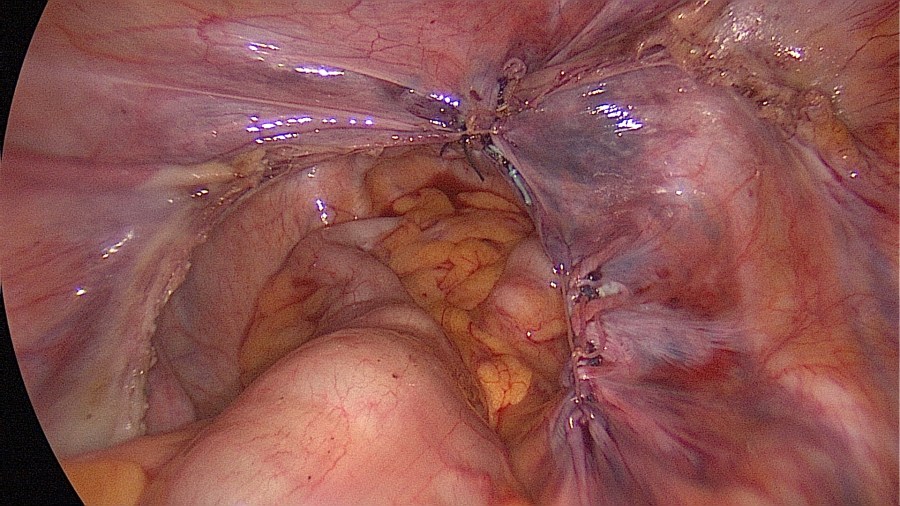
Peritonization and complete covering of the mesh. 
Morcellation of the uterine corpus. If a fixation of the sigmoid colon was performed, remember to untie this fixation before initiating the morcellation. 
Closure of the fascia along with the peritoneum at the site where the power morcellator was used. 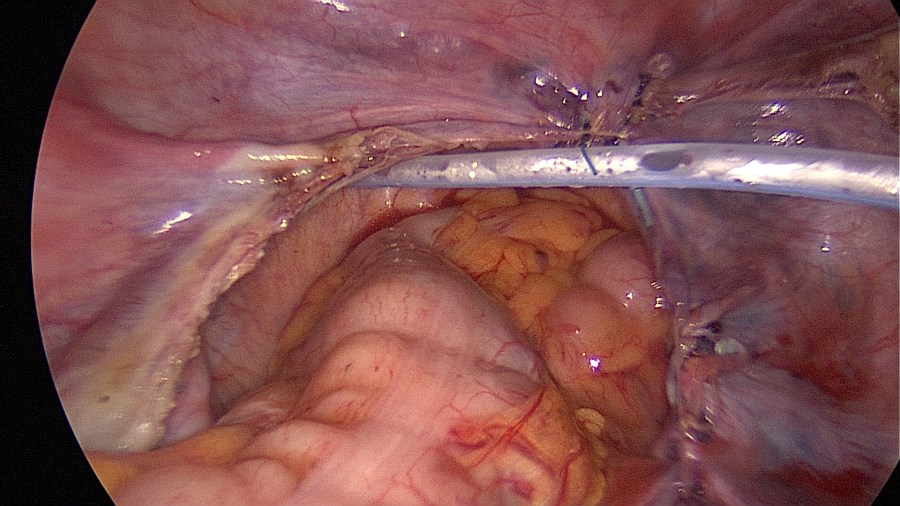
Placement of a drainage (optional).
Contraindications
- Gynecological malignancy or suspicious cytology from the cervix.
- Patient desires future pregnancy.
- Laparoscopy is contraindicated.
Complications
- Big vessel injury and bleeding.
- Injury of the right ureter, the sigmoid colon, or the bladder.
- Lumbar spondylodiscitis.
- De novo stress urinary incontinence.
Postoperative Management
- Removal of transurethral urinary catheter (duration maximum 24 hours unless concomitant colporrhaphy was performed).
- Removal of vaginal packing if concomitant colporrhaphy was performed.
- Low-Molecular-Weight-Heparin (LMWH) once daily.
- Control residual bladder volume, perform nephrosonography and inspect the wound before discharge.
- Postoperative restrictions for 6 weeks.
- Follow-up in 6-8 weeks.
Bibliography
- Rosati, M., Bramante, S., Bracale, U., Pignata, G., & Azioni, G. (2013). Efficacy of laparoscopic sacrocervicopexy for apical support of pelvic organ prolapse. JSLS : Journal of the Society of Laparoendoscopic Surgeons, 17(2), 235–244. https://doi.org/10.4293/108680813X13654754535115
- Qu, D. C., Chen, H. B., Yang, M. M., & Zhou, H. G. (2019). Management of lumbar spondylodiscitis developing after laparoscopic sacrohysteropexy with a mesh: A case report and review of the literature. Medicine, 98(49), e18252. https://doi.org/10.1097/MD.0000000000018252

1 Comment