
Surgical Treatment of Stress Urinary Incontinence
The patient’s reduced quality of life is the indication for treatment of stress urinary incontinence. Failed conservative treatment may lead to surgical treatment options.
Treatment Options
Retropubic midurethral sling, autologous rectus fascial sling and colposuspension are all validated surgical treatments for stress urinary incontinence. Although there are plenty of options, sometimes alternatives are sought. This can be due to procedure-related risks, comorbidities, unfavorable factors like intrinsic sphincter deficiency and fixed urethra, or failed previous surgical treatment (1).
Bulking agents
Bulking agents to treat stress urinary incontinence appeared as early as 1938, when Murless injected sodium morrhuate into the anterior vaginal wall (2). Over the years they have proven themselves as a minimally invasive treatment with rapid recovery and a low morbidity rate (1). As patients become more informed of the potential side effects of meshes, they may opt for injections of bulking agents even if the chance of cure is reduced (2).
Bulkamid®
Polyacrylamide hydrogel (Bulkamid®) was introduced in Europe in 1996. It is considered a safe intervention for treating women with stress urinary incontinence. Sometimes repeat injections may be required (3). Concerning the outcome, a prospective multicenter study in the U.S. with 229 patients treated with Bulkamid® reported that 47,2% of them had no incontinence episodes and 77,1% of them felt cured or improved after 1 year (4).
Technique
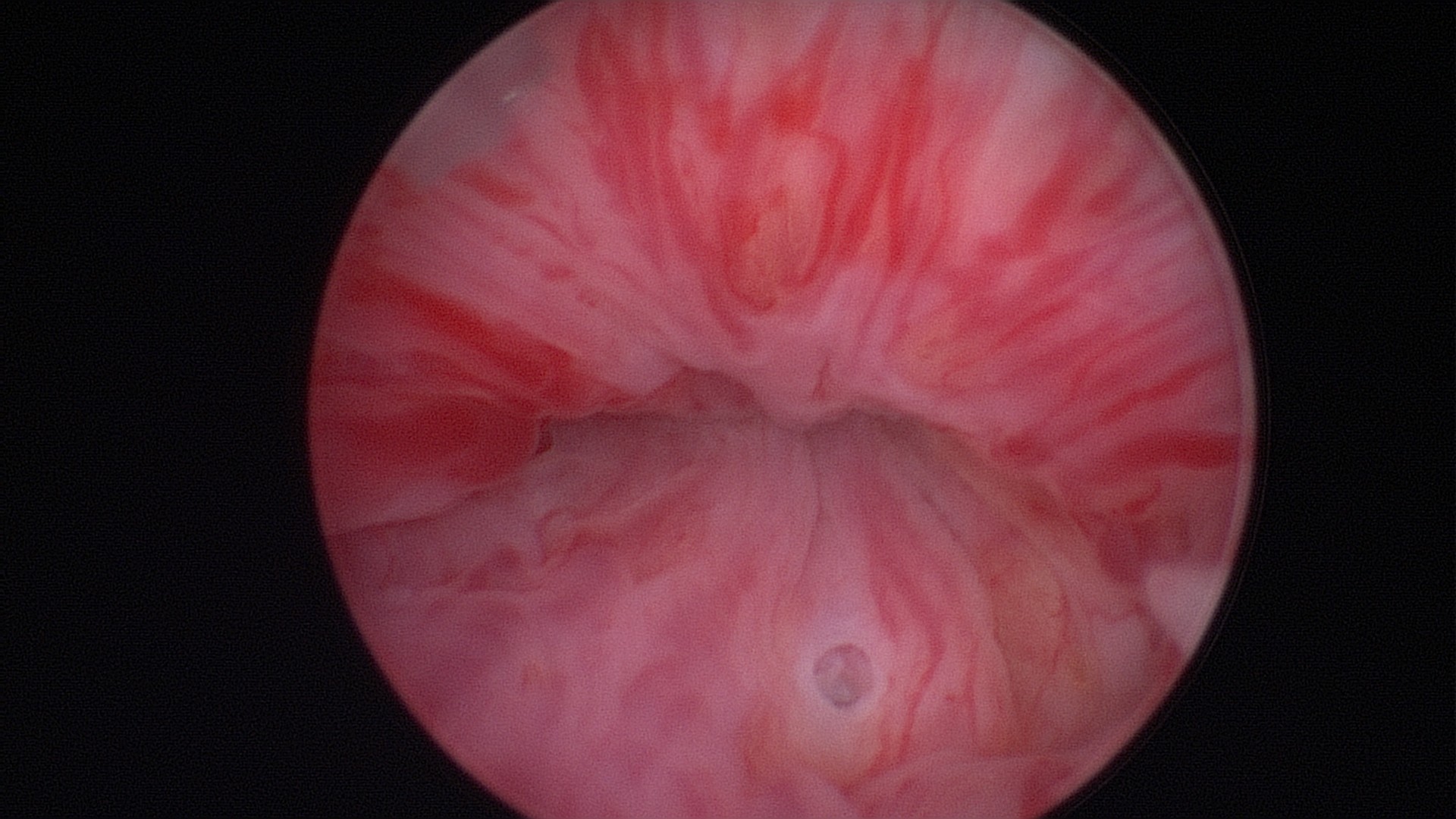
Beginn with a thorough cystoscopy. Patients that have incontinence recurrence should be examined for sling or even suture erosion. Watch out for tumors or stones. 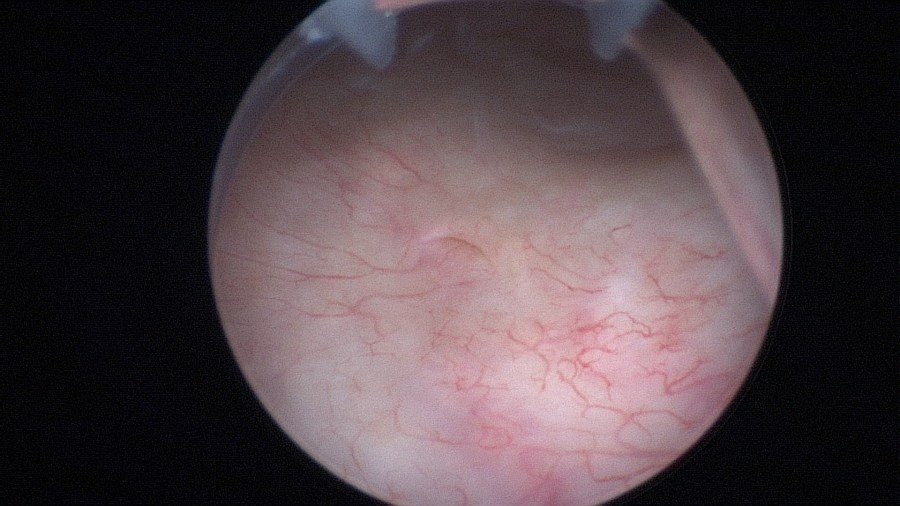
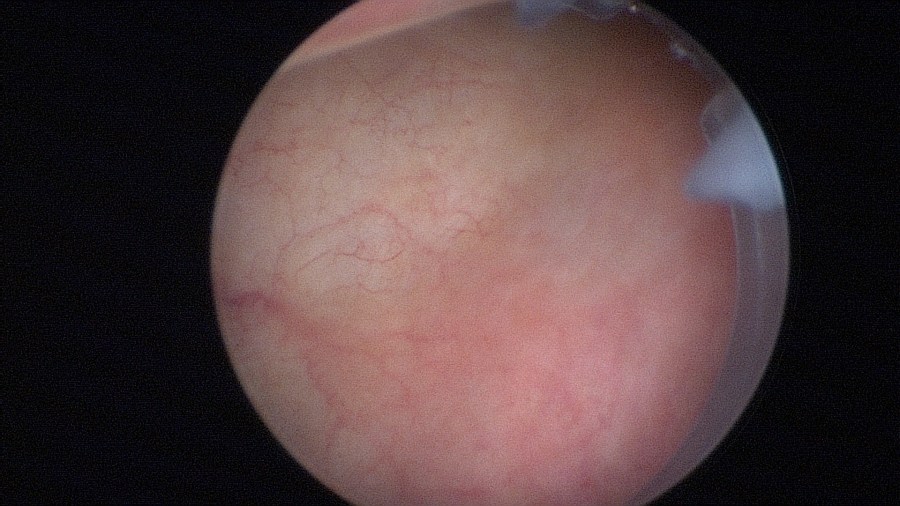
Documentation of the right ureteral orifice. 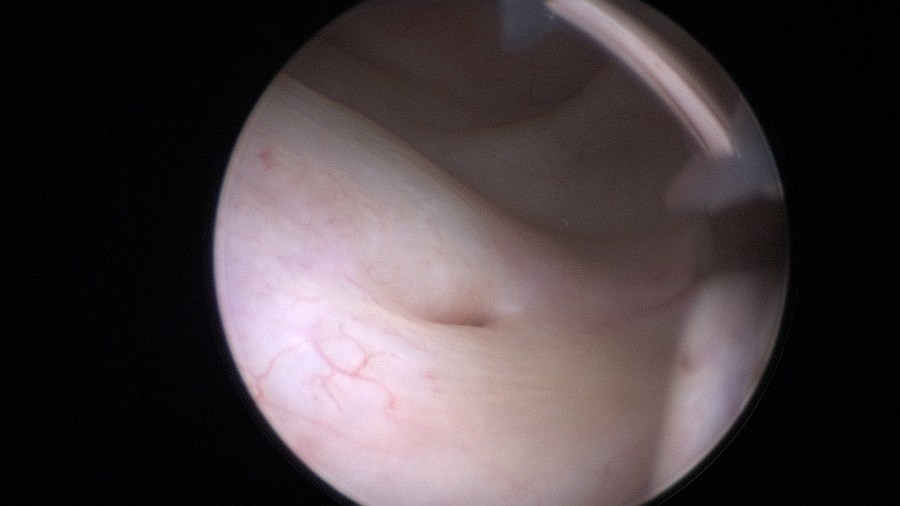
Documentation of the left ureteral orifice. 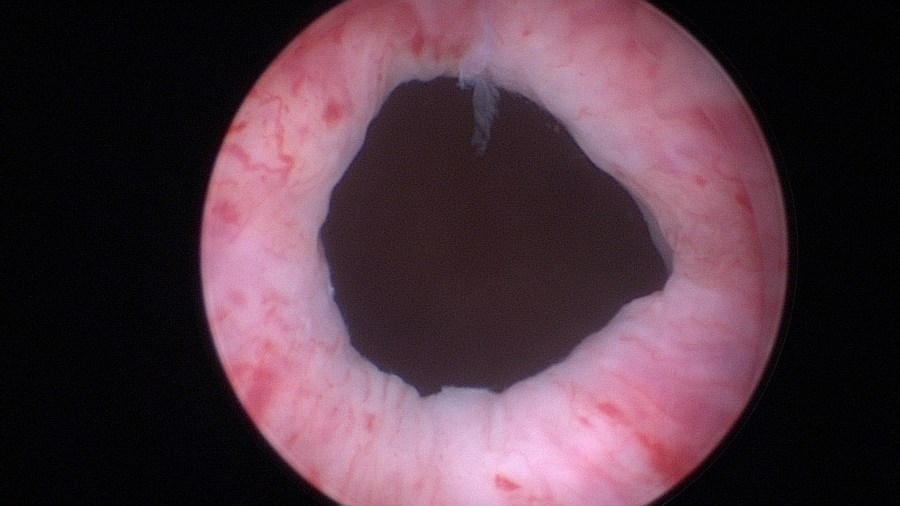
The bladder neck. 
The mid-urethra. 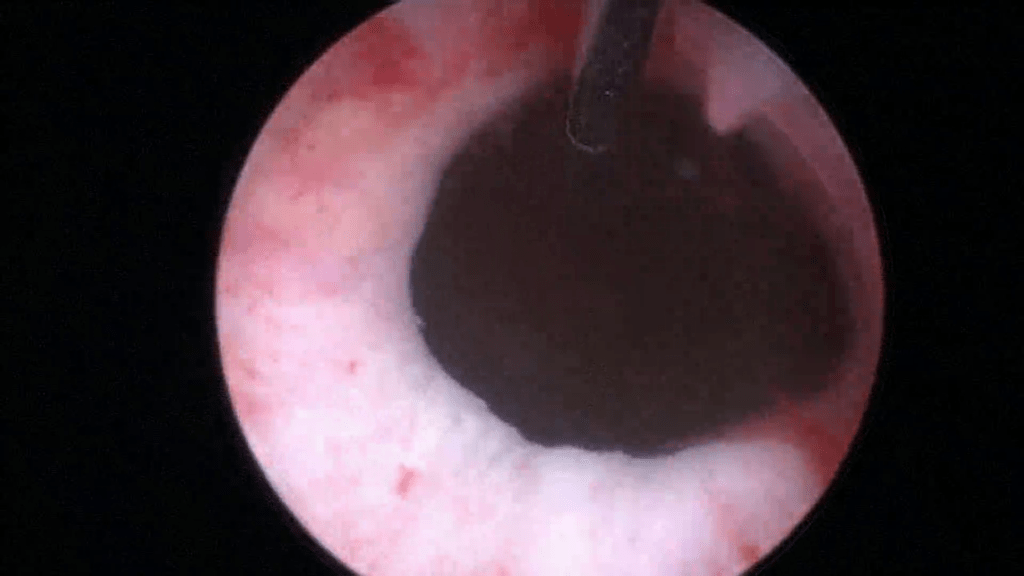
Pushing the needle forward up to the second marking (2cm mark) gives you perspective of actual distance. 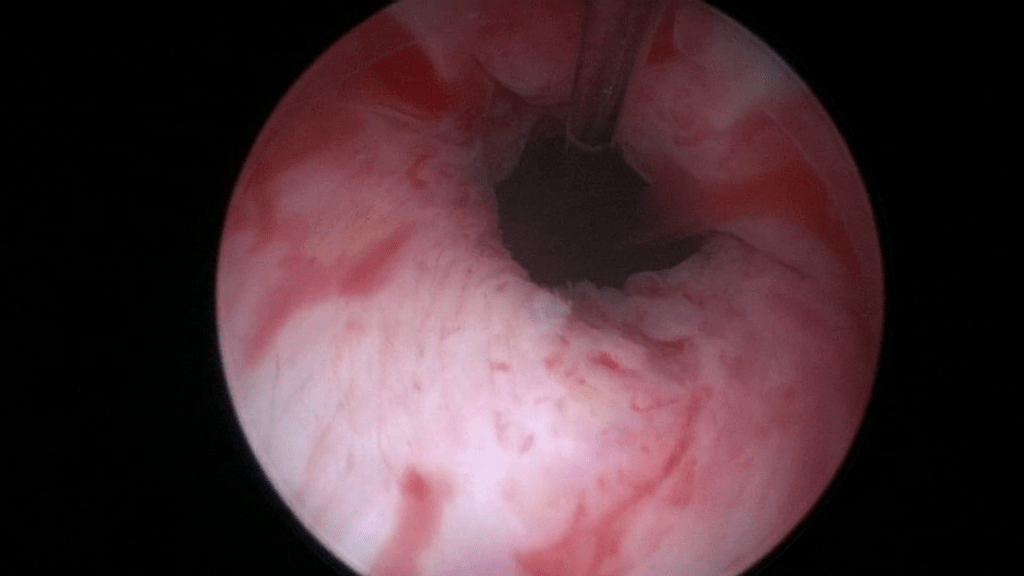
By retracting the cystoscope you can perform an accurate measurement – estimate of the urethra. 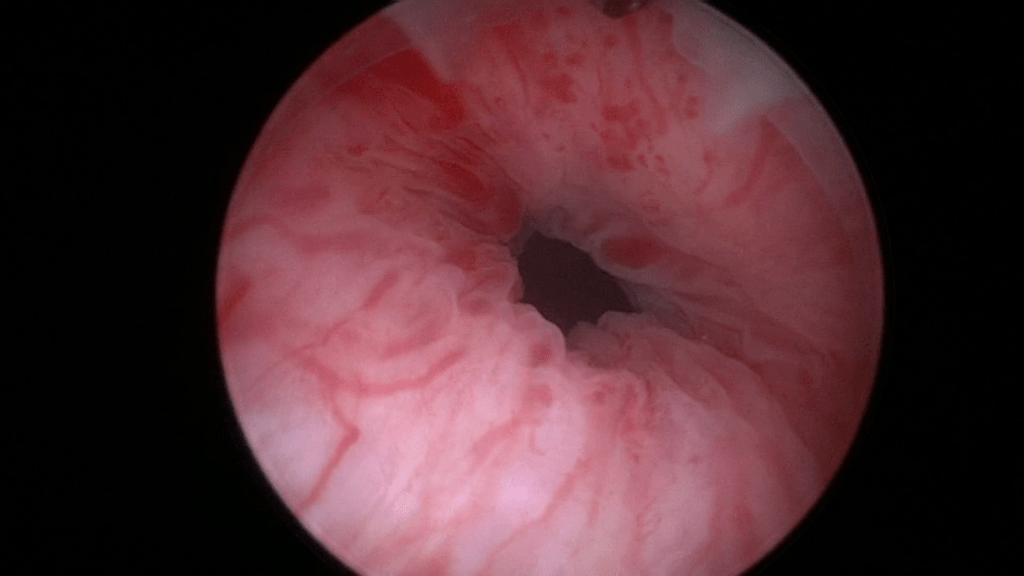
The right height to insert the needle is at least 2cm from the bladder neck. This is because after inserting you push the needle up to the first mark (1cm). In other words you are placing the depots 1cm higher than the actual location of the cystoscope. 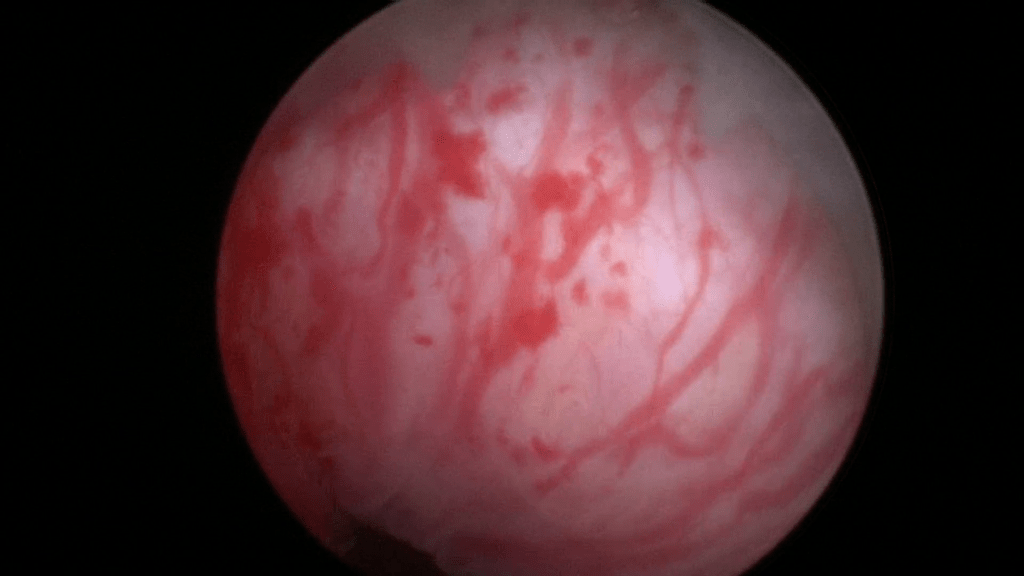
Start on the 12 o’clock position and gently press the cystoscope against the anterior urethral wall while making sure its axis remains parallel to the urethra. This will create a small “mucosal shelf”, in which the needle can vertically penetrate the urethra. 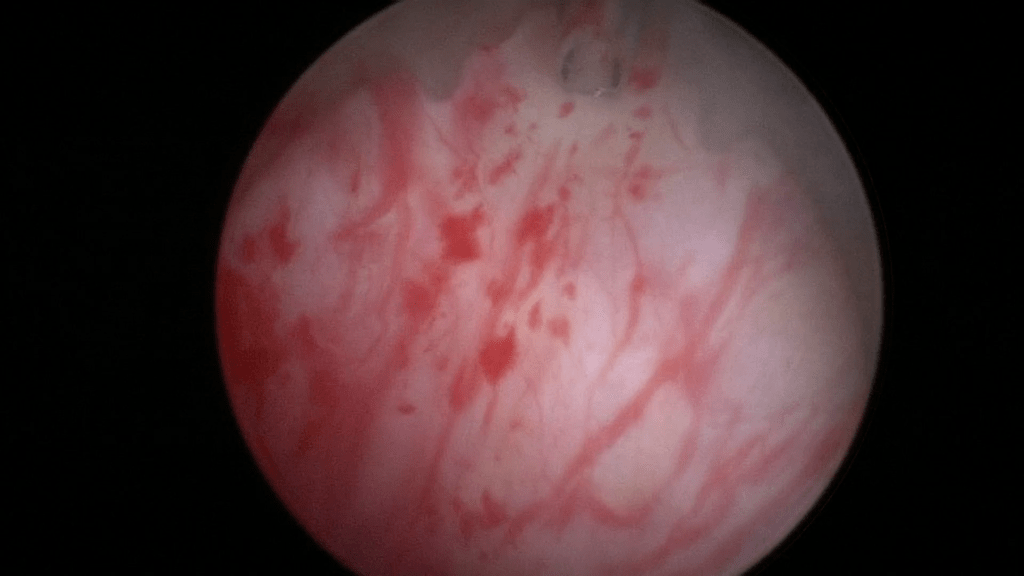
The bevel of the needle should be facing towards the center of the lumen. 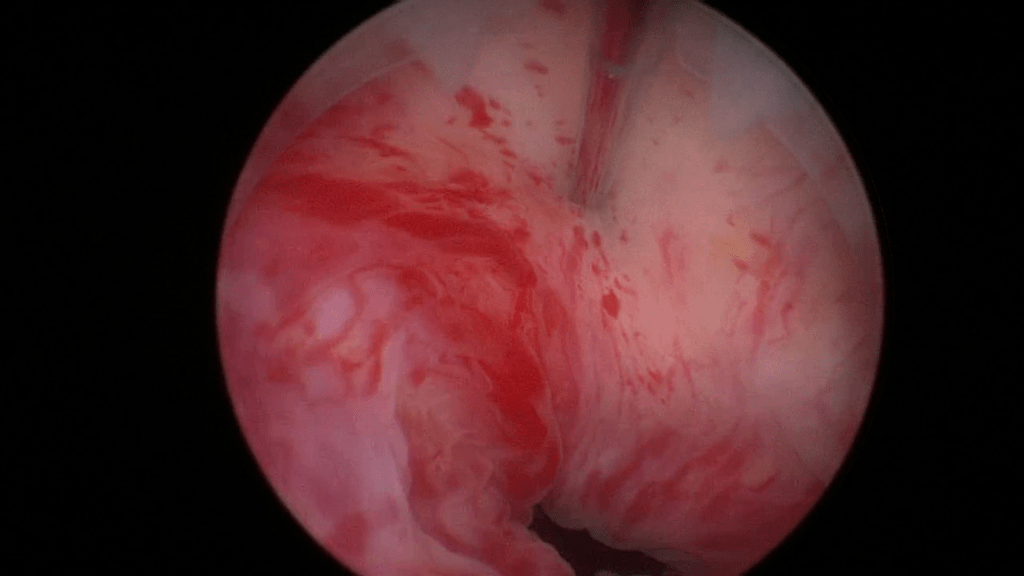
Insert the needle up to the 1cm mark. 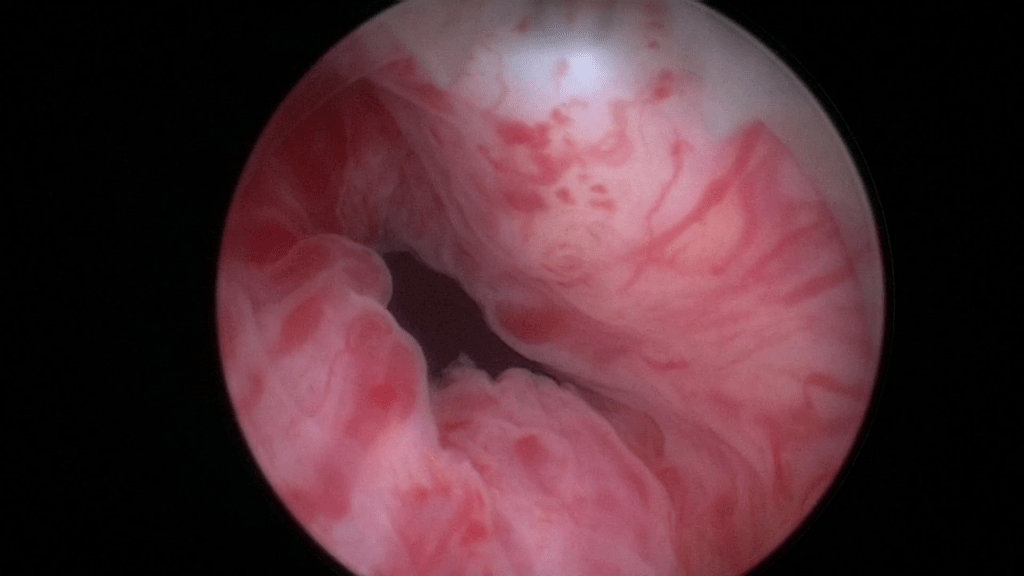
Begin injecting Bulkamid® hydrogel. 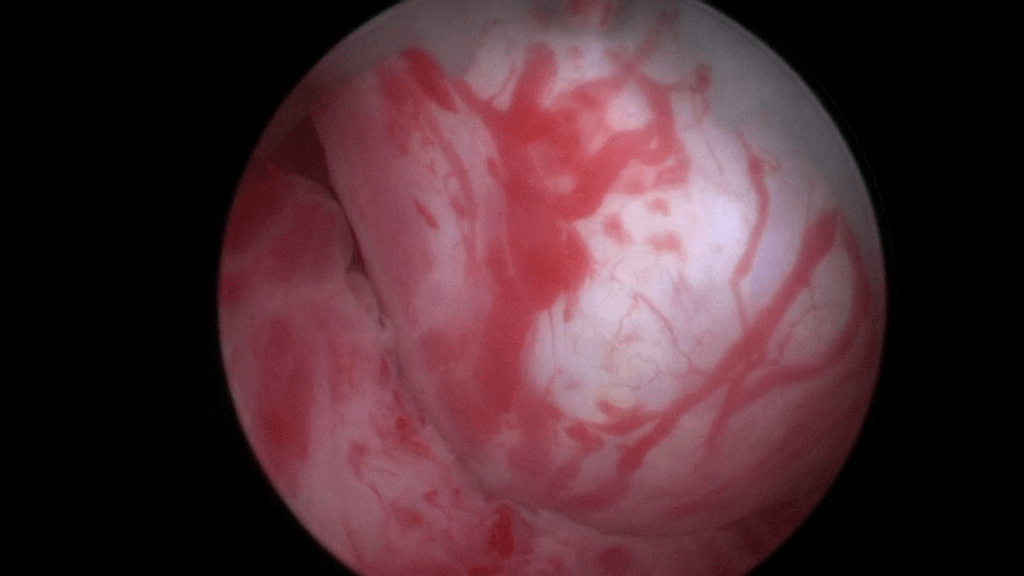
Image after injecting 0.5ml at the 12 o’clock position. 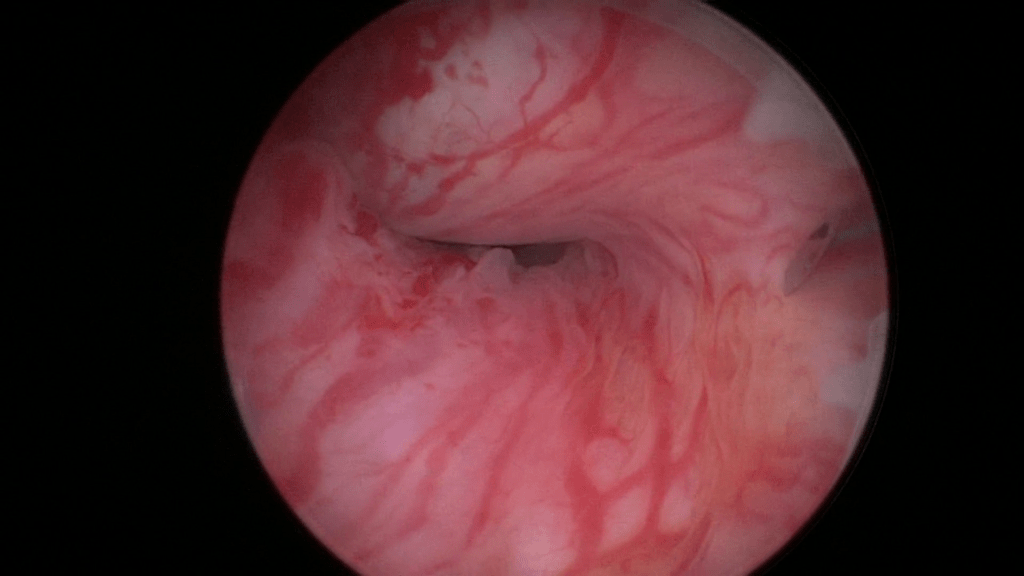
Rotate the sheath and inject now at the 3 o’clock position. Again notice that the bevel of the needle faces the center of the lumen and that an adequate “mucosal shelf” is formed. 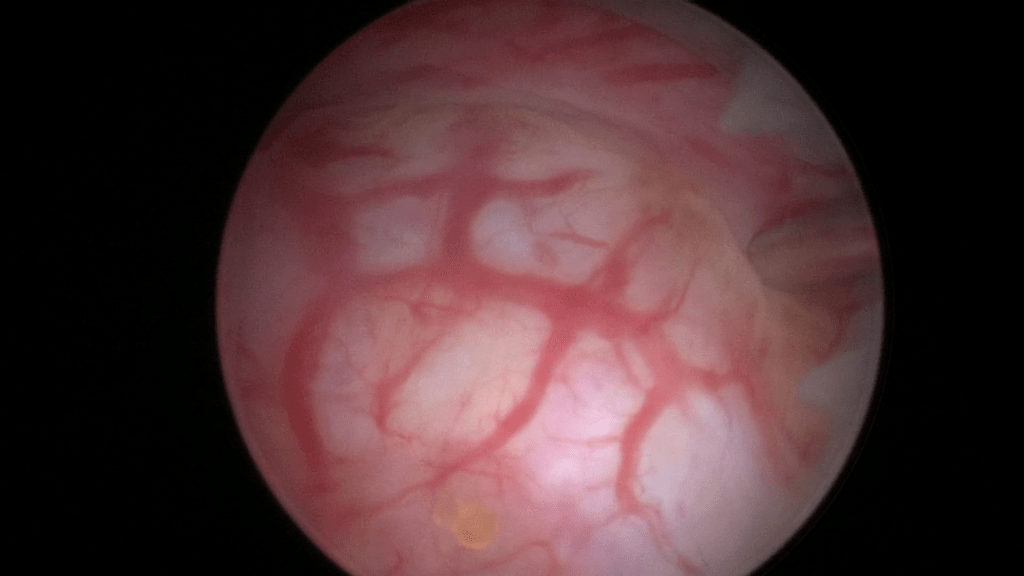
Image after injecting the second 0.5ml of Bulkamid® hydrogel at the 3 o’clock position. 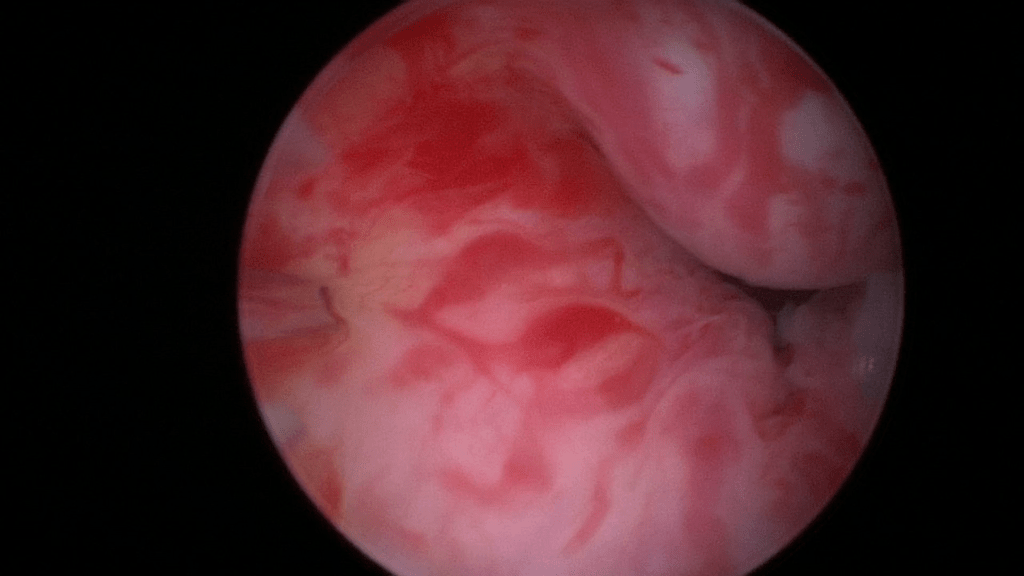
The needle is shortly removed and the second syringe of 1ml Bulkamid® hydrogel is loaded. Find the exact location of the previous injections and continue with the next one at 9 o’clock. 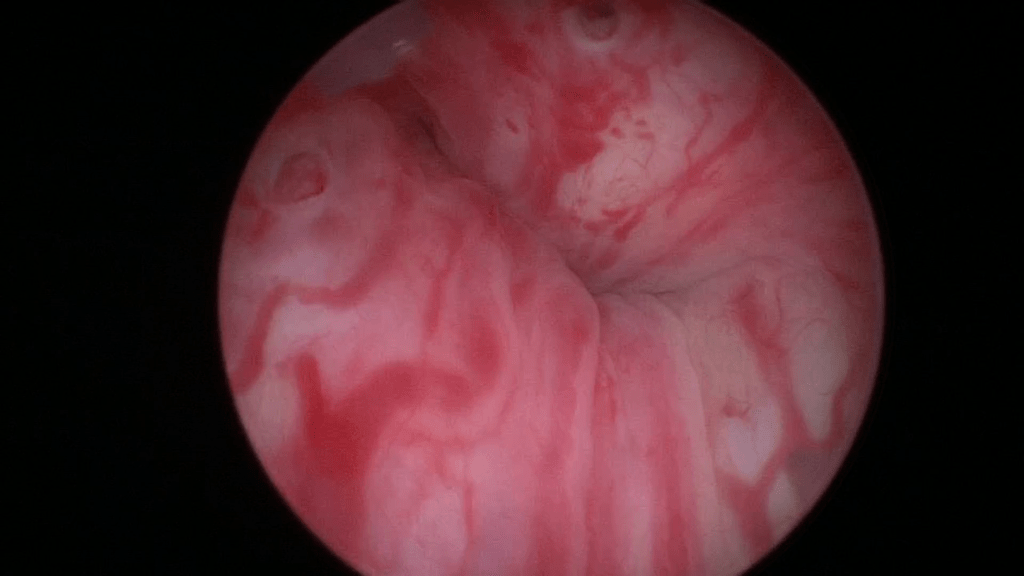
Image after injecting the third 0.5ml Bulkamid® hydrogel at 9 o’clock. 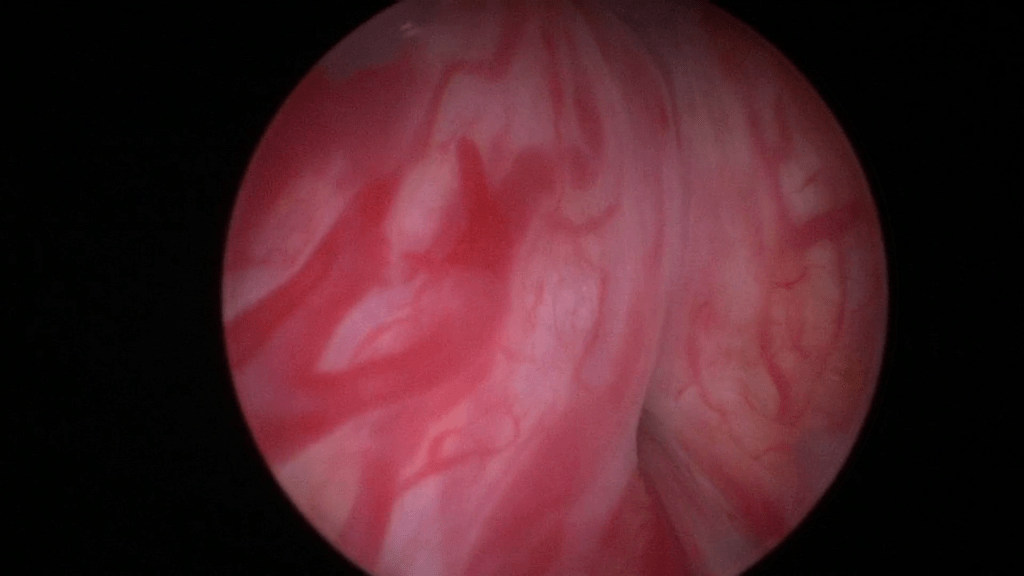
Lastly inject the final 0.5ml of Bulkamid® hydrogel at the 6 o’clock position. 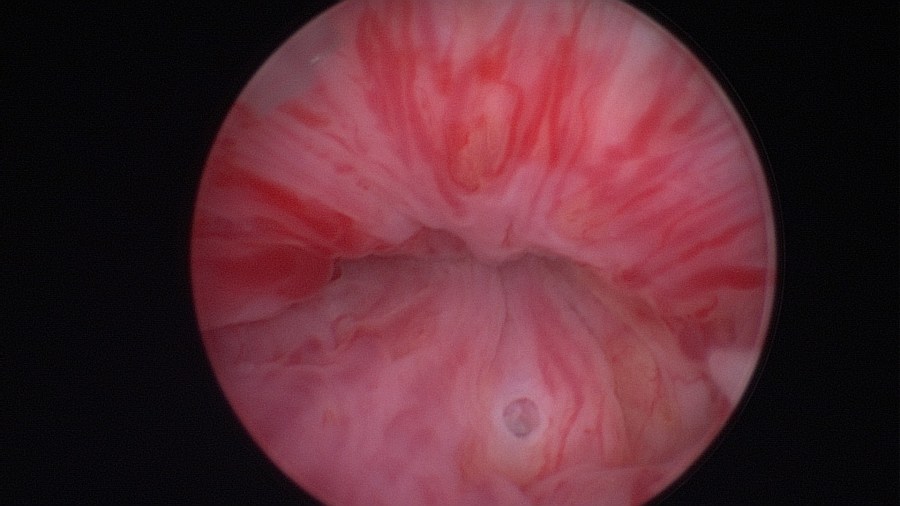
Final image of the mid-urethra after creating four depots of Bulkamid® at the 12, 3, 9 and 6 o’clock positions.
Watch the video of a transurethral injection on youtube by clicking here.
Complications
- Pain at the injection site.
- Urinary tract infection.
- Temporary urinary retention, outlet obstruction.
- Transient hematuria.
- Prolapse of the urethral mucosa.
- Bladder masses.
- Extremely rare: periurethral abscess (2).
Postoperative Management
- Sonographic documentation of residual bladder volume.
- Sonographic documentation of depots.
- Early discharge.
- Postoperative restrictions for 2 weeks.
- Consider laxatives to avoid straining.
- Follow-up in 6 weeks.
Bibliography
- Matsuoka, P. K., Locali, R. F., Pacetta, A. M., Baracat, E. C., & Haddad, J. M. (2016). The efficacy and safety of urethral injection therapy for urinary incontinence in women: a systematic review. Clinics (Sao Paulo, Brazil), 71(2), 94–100. https://doi.org/10.6061/clinics/2016(02)08
- Hussain, SM, Bray, R. Urethral bulking agents for female stress urinary incontinence. Neurourology and Urodynamics. 2019; 38: 887– 892. https://doi.org/10.1002/nau.23924
- Kasi, A.D., Pergialiotis, V., Perrea, D.N. et al. Polyacrylamide hydrogel (Bulkamid®) for stress urinary incontinence in women: a systematic review of the literature. Int Urogynecol J 27, 367–375 (2016). https://doi.org/10.1007/s00192-015-2781-y
- Sokol, E.R., Karram, M.M., & Dmochowski, R. (2014). Efficacy and Safety of Polyacrylamide Hydrogel for the Treatment of Female Stress Incontinence: A Randomized, Prospective, Multicenter North American Study. Journal of Urology, 192(3), 843–849. https://doi.org/10.1016/j.juro.2014.03.109
