
Indication
- The main condition is that the patient desires to preserve her childbearing potential.
- The main indication is intramural or subserosal fibroids causing serious symptoms (excessive menstrual bleeding, pelvic pain or pressure).
Only the removal of submucosal fibroids has been consistently shown to improve fertility outcomes.
Technique
- Preoperative antibiotic prophylaxis (single shot, second generation cephalosporine).
- Patient in lithotomy position.
- Desinfection of the abdomen, thighs, vulva and vagina.
- Sterile surgical drapes.
- Urinary catheter.
- Examination under anesthesia.
- Use of an atraumatic uterine manipulator that allows chromopertubation.
- Change of surgical gloves, start of laparoscopy.
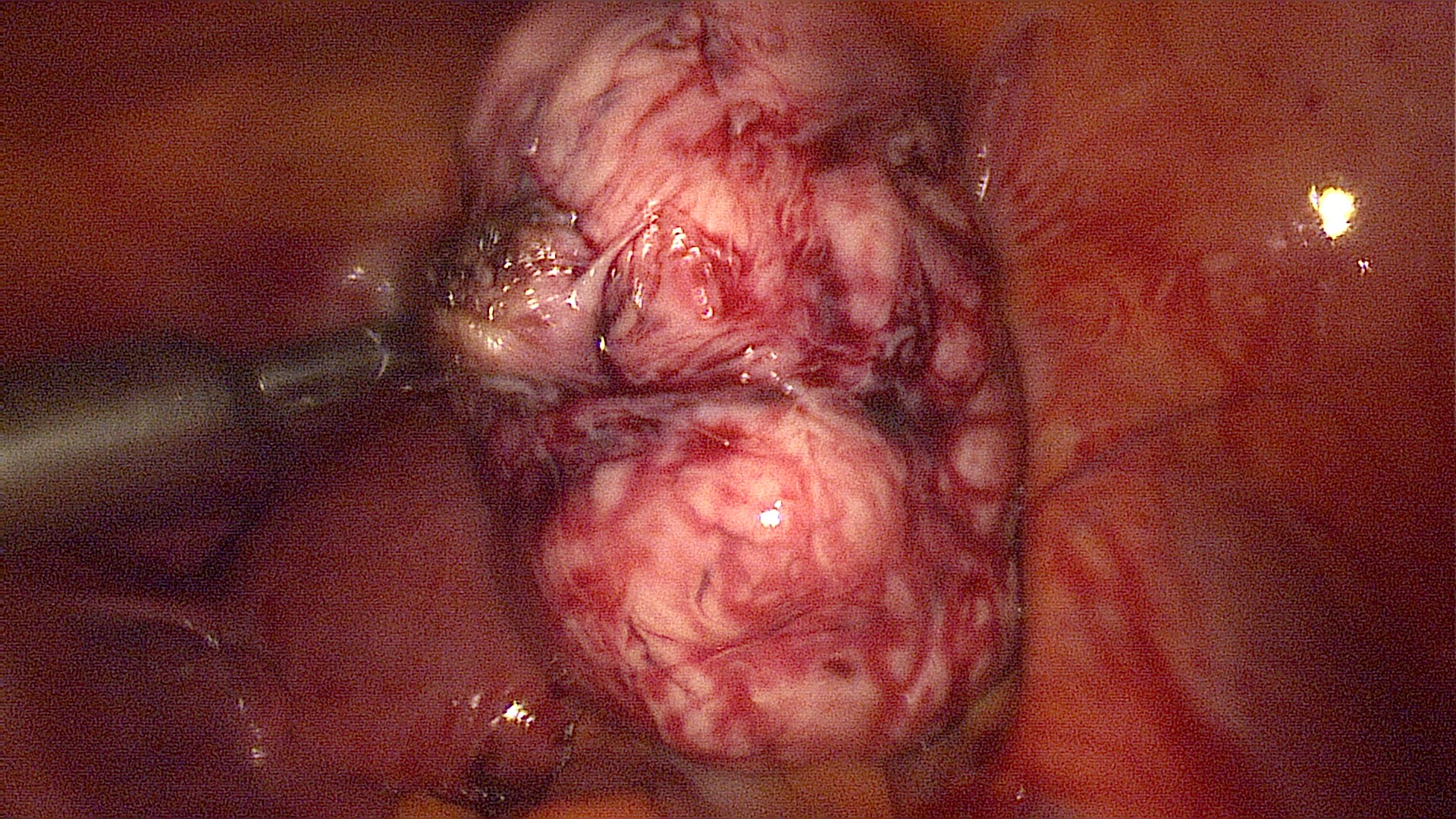
Demonstration of the uterus and identification of the fibroid(s) that is to be removed. This patient has a 7cm intramural fibroid inside the posterior uterine wall. 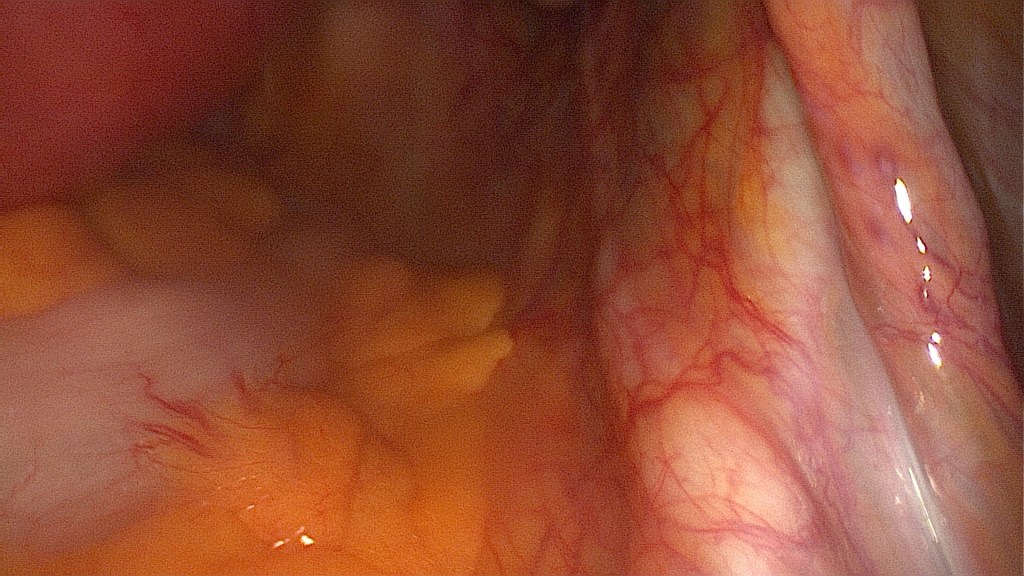
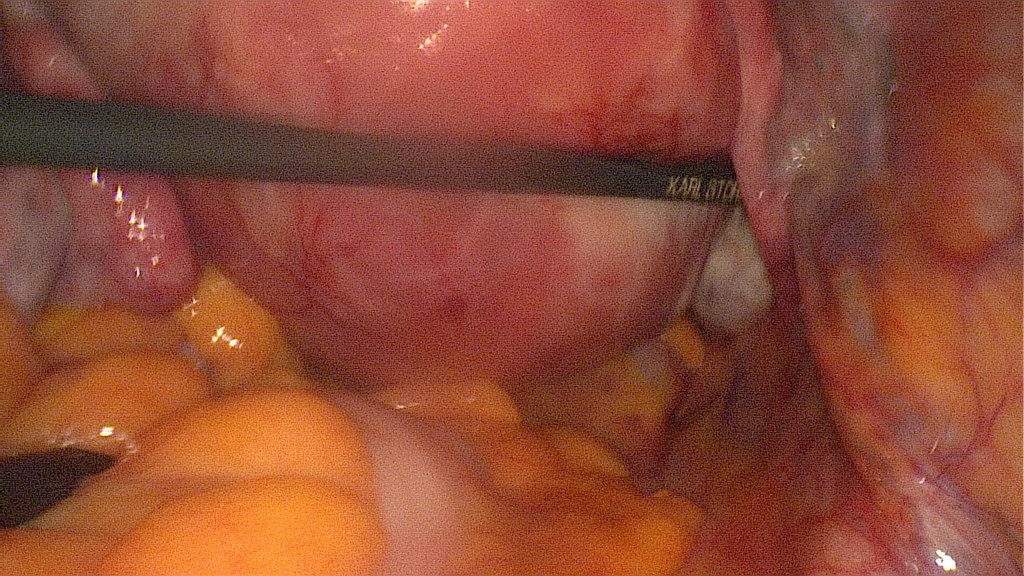
Identification of the right ureter. 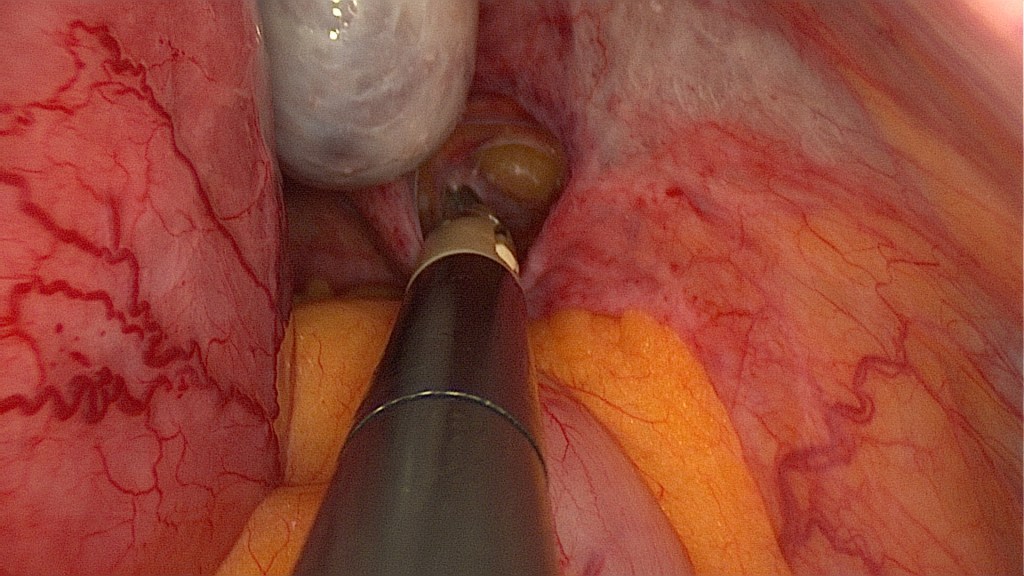
Following the ureter to where it crosses the extension of the medial umbilical ligament helps directly identify the location of the origin of the ipsilateral uterine artery. Opening of the retroperitoneum. 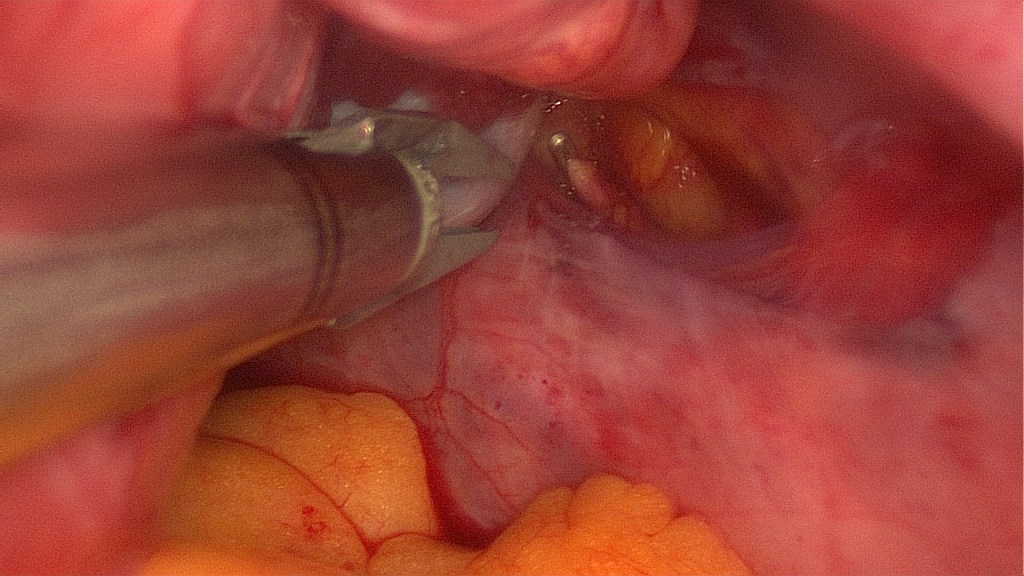
Placement of a non-permanent titanium clip on the right uterine artery. 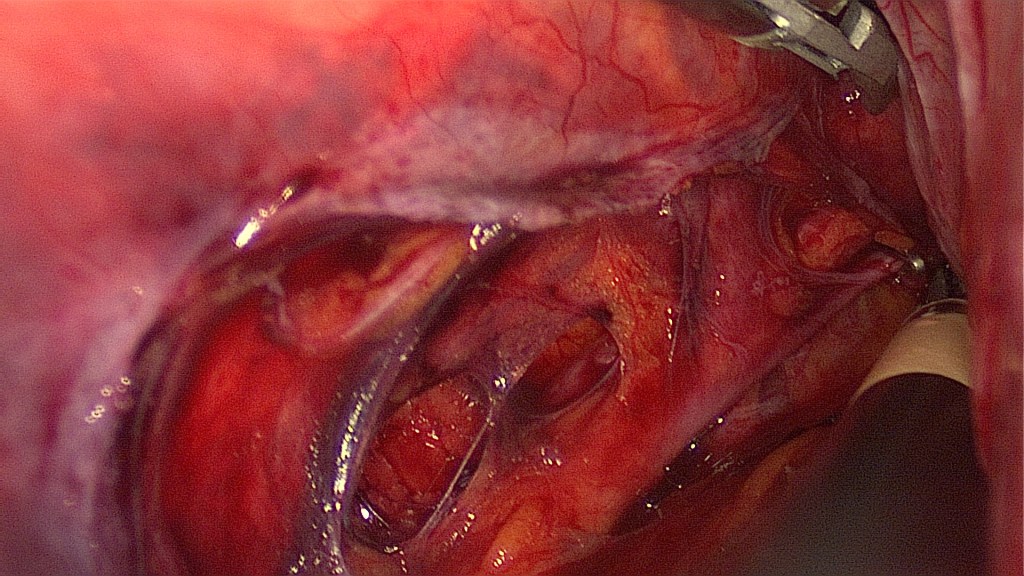
In case the transperitoneal visualization of this specific area is not accurately possible, a bigger opening of the retroperitoneal space may be made, like on this patient’s left side. 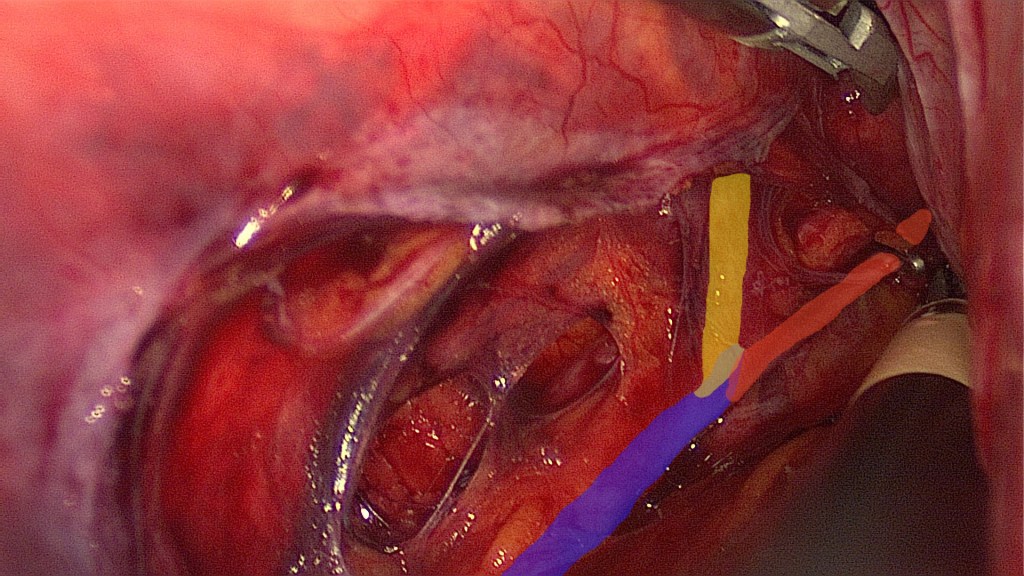
This is the same as the previous image. Blue: left internal iliac artery. Yellow: left internal iliac artery after branching of the uterine artery. Red: left uterine artery with a placed titanium clip. 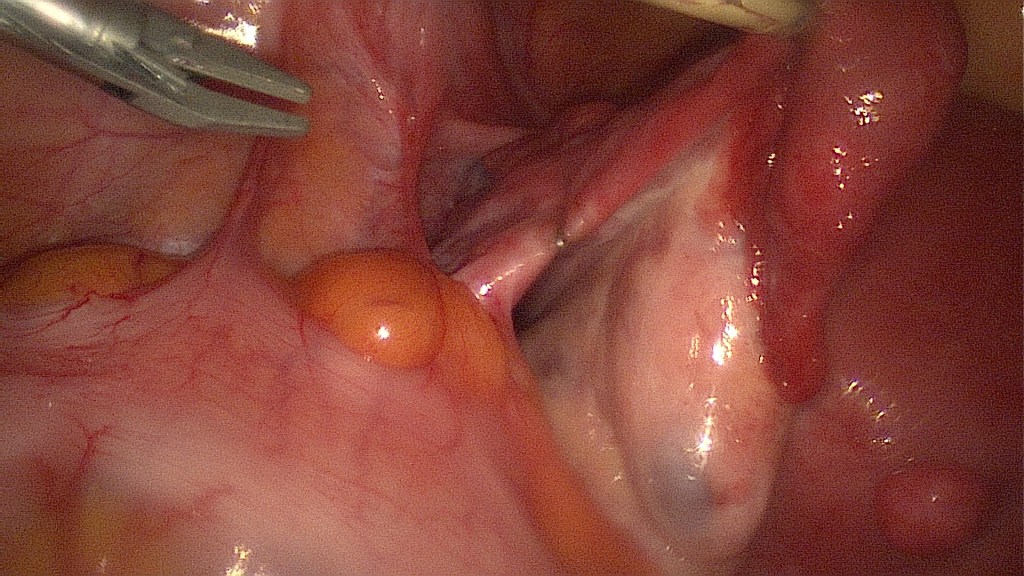
Clipping of the left IP ligament (ovarian artery). 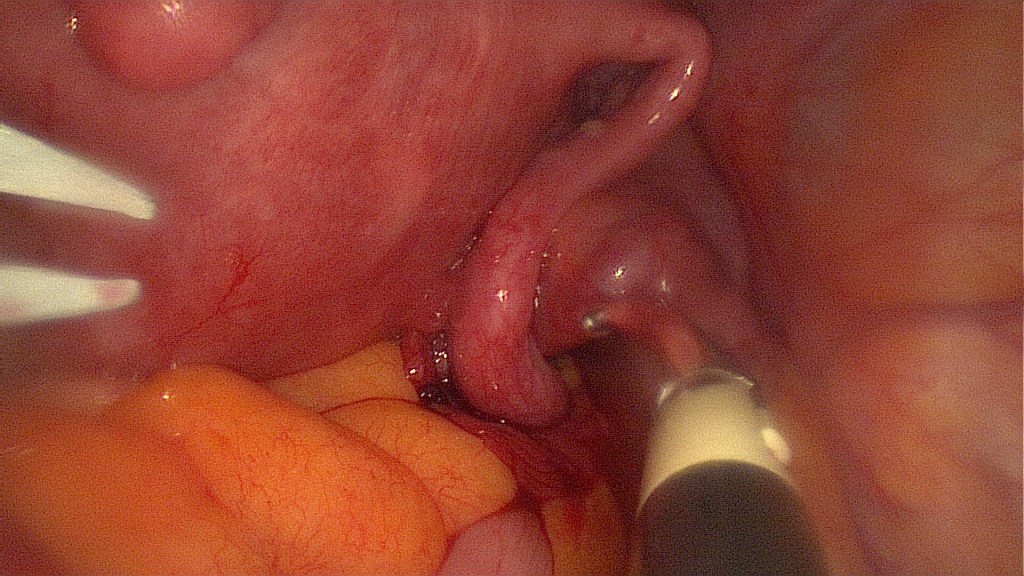
Clipping of the right IP ligament (ovarian artery). 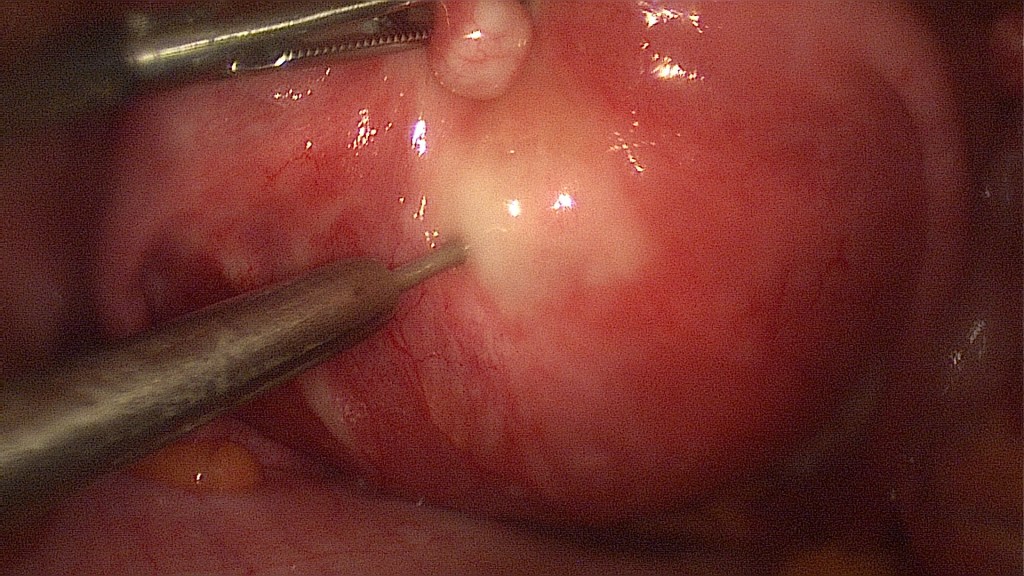
Injection of diluted epinephrine. 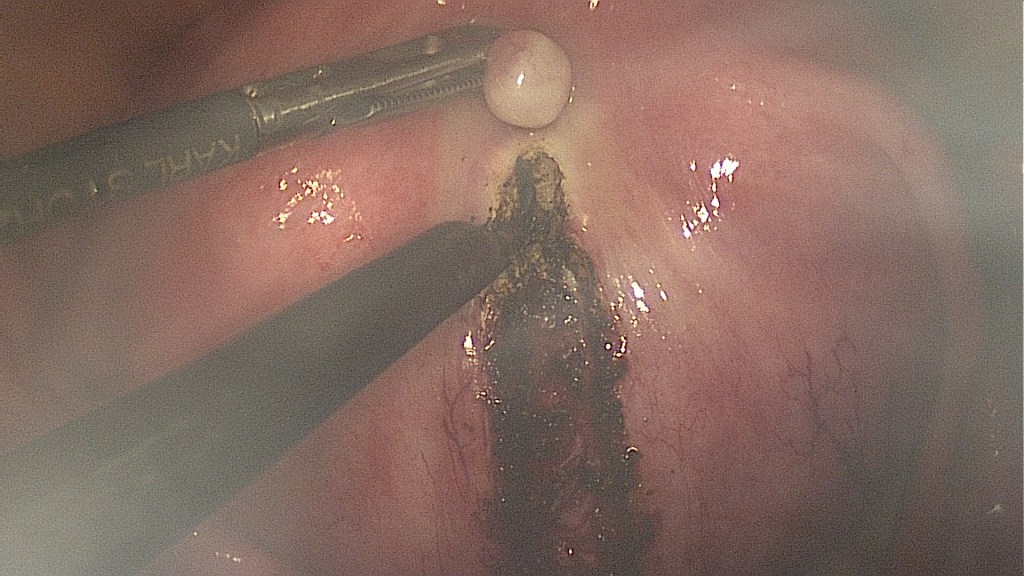
Monopolar cautery is used to perform a medial vertical incision above the highest point of the fibroid. 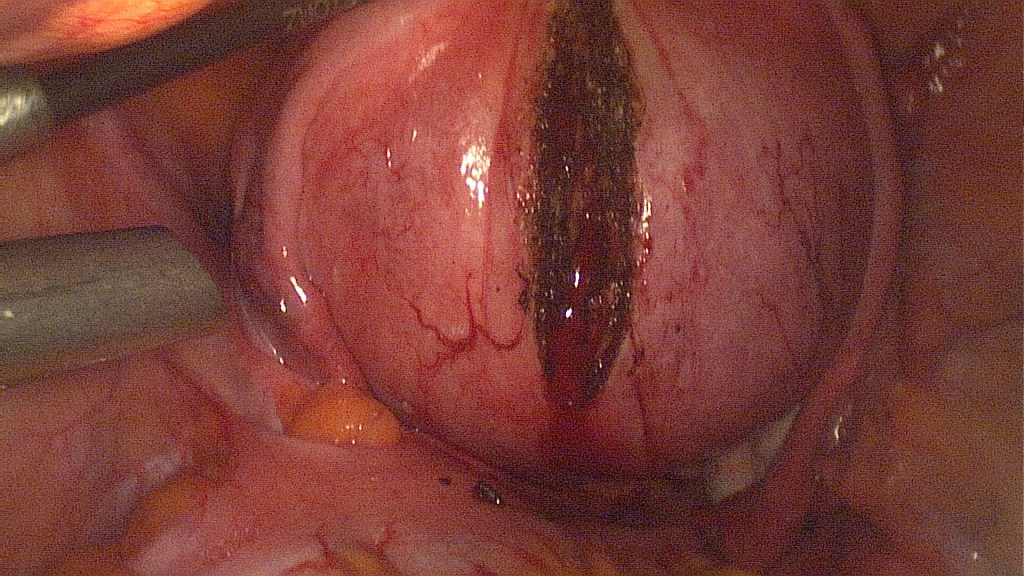
Note the minimal bleeding. 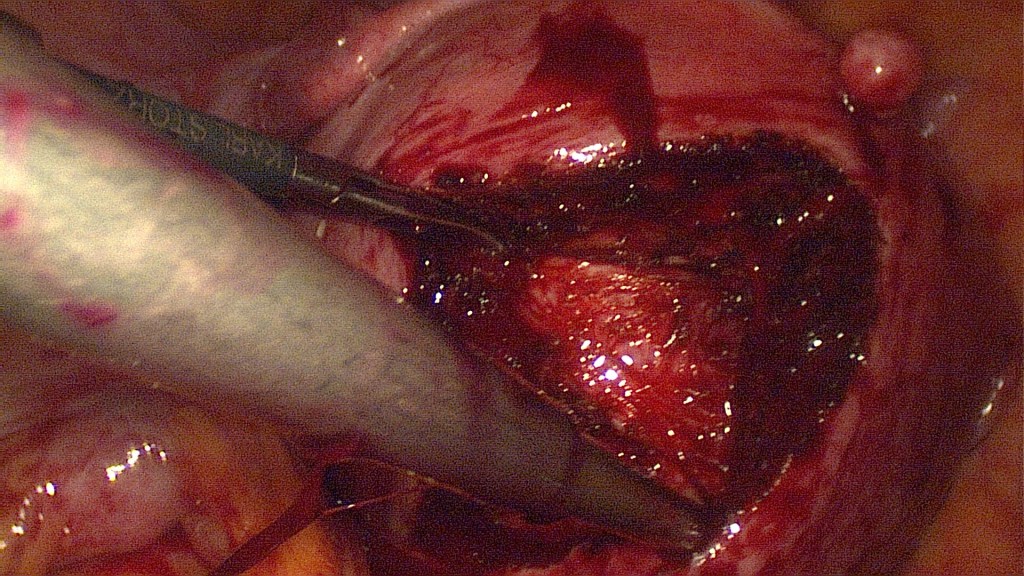
Identification of the myoma capsule. 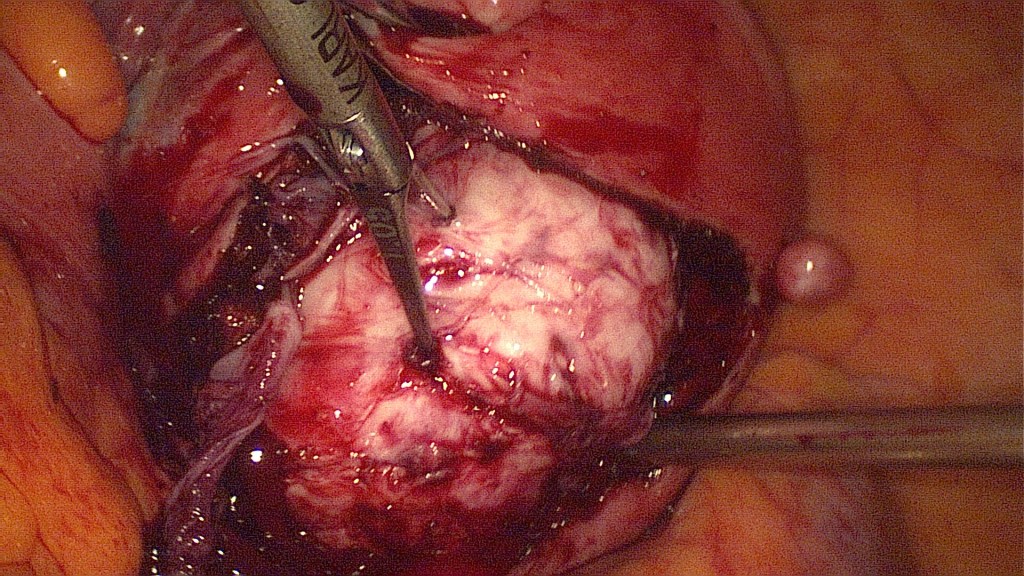
Grasping of the myoma with the bullet forceps and use of careful traction and counter-traction. 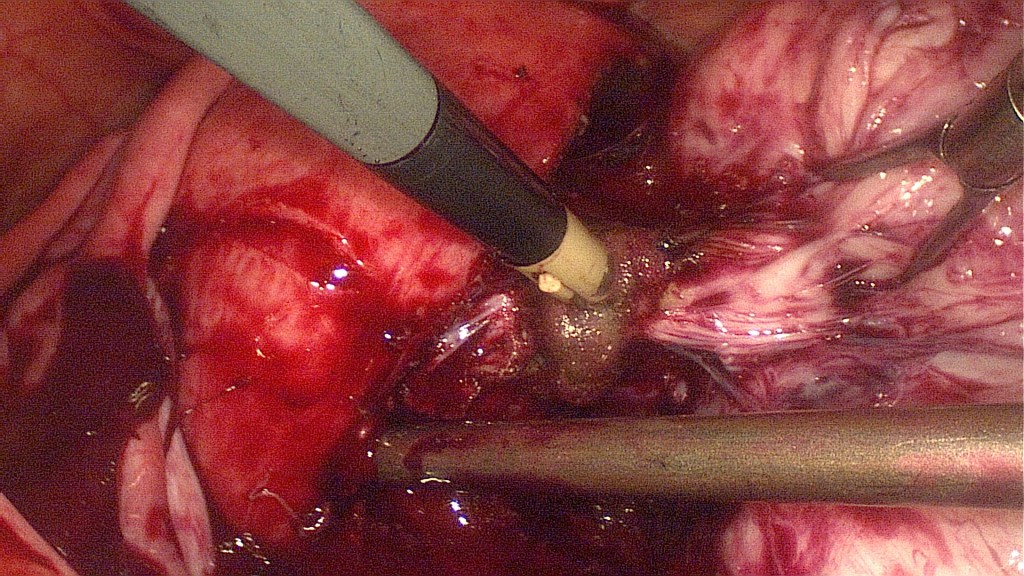
Bipolar coagulation and cutting of the vascular pedicle in the base of the myoma. 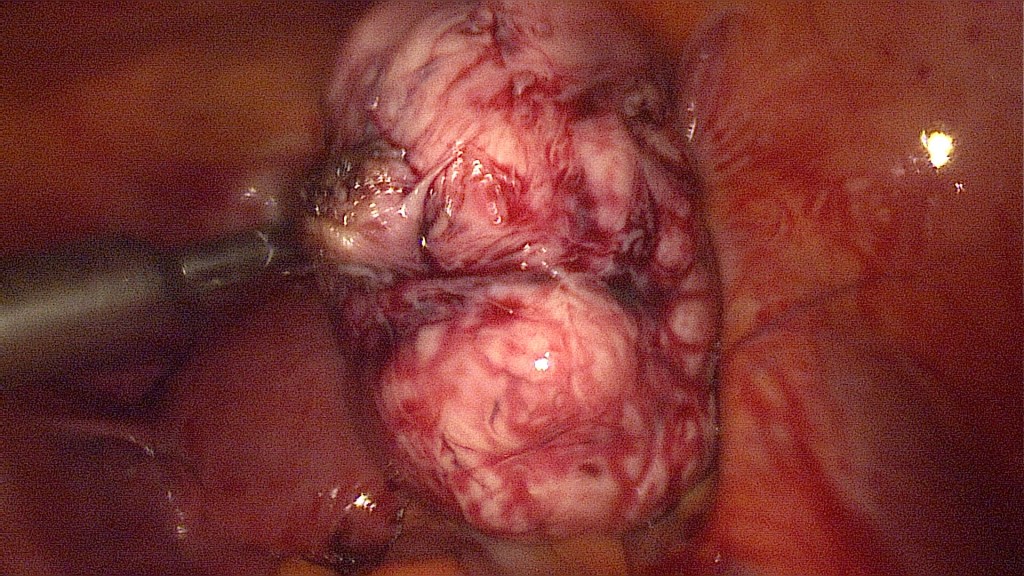
The 7cm myoma has been fully enucleated. 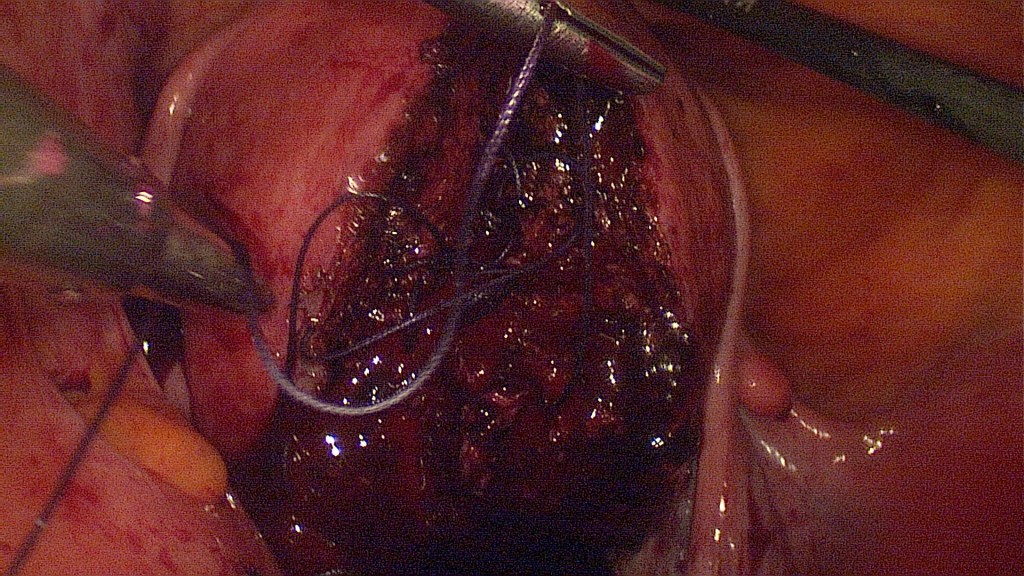
Without the use of excessive bipolar coagulation, begin of the suturing. The chromopertubation showed no opening of the uterine cavity. 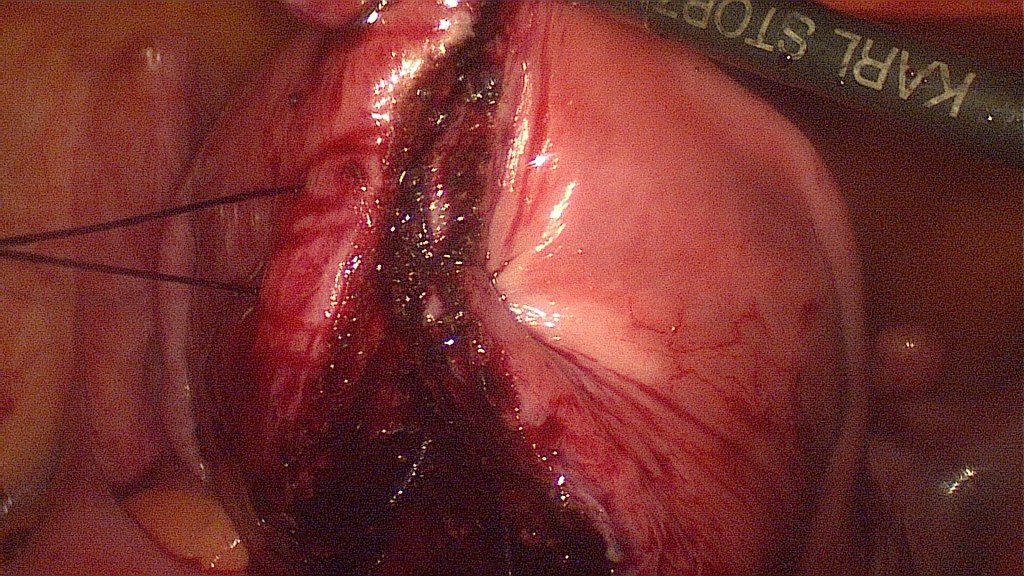
The uterine wall has been sutured in two layers with a continuous, vicryl 0 suture. A third layer with interrupted, PDS, figure of 8 sutures reassures the uterine integrity. 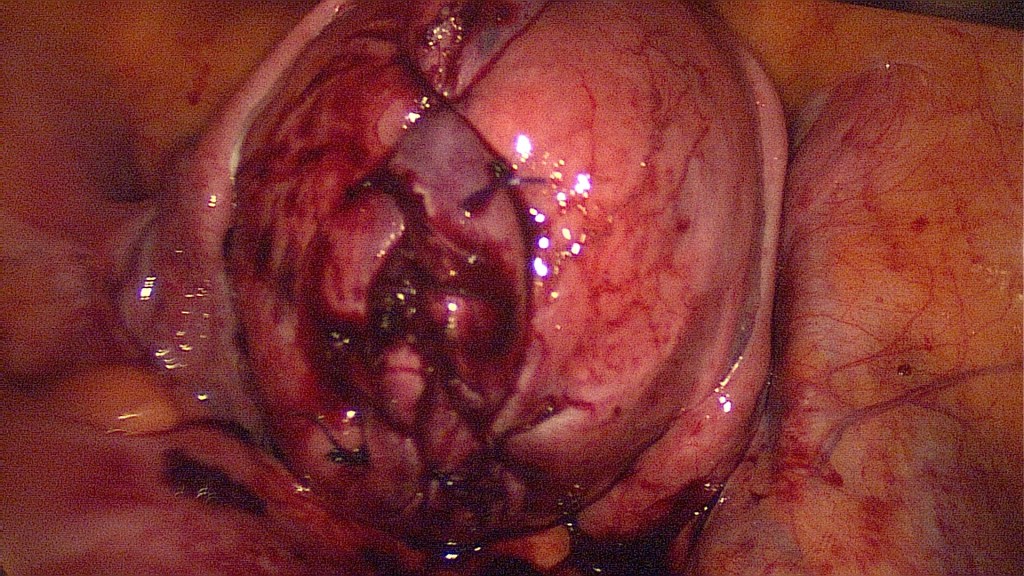
Final view of the uterus. 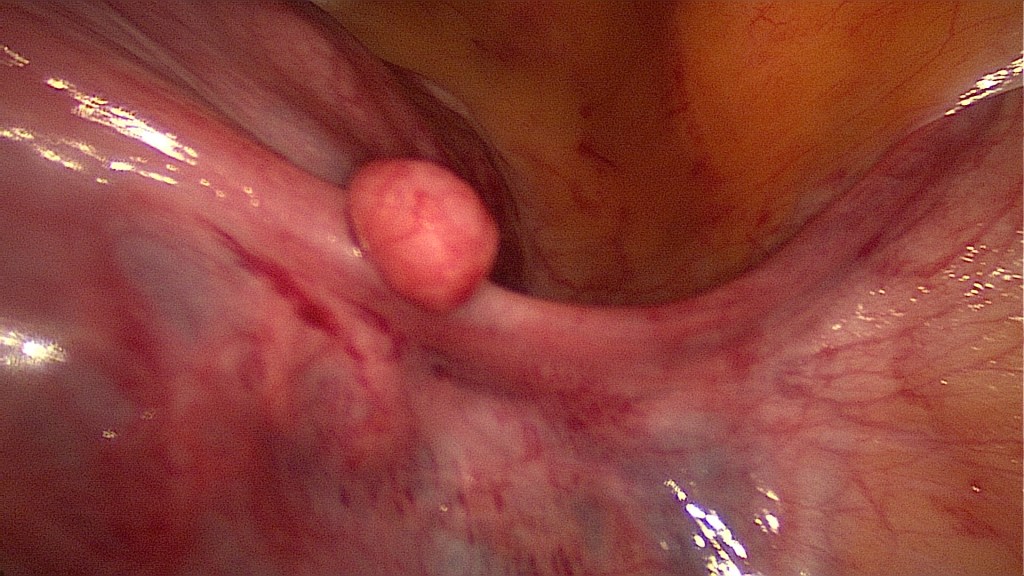
Now is the time to remove any further myomas. 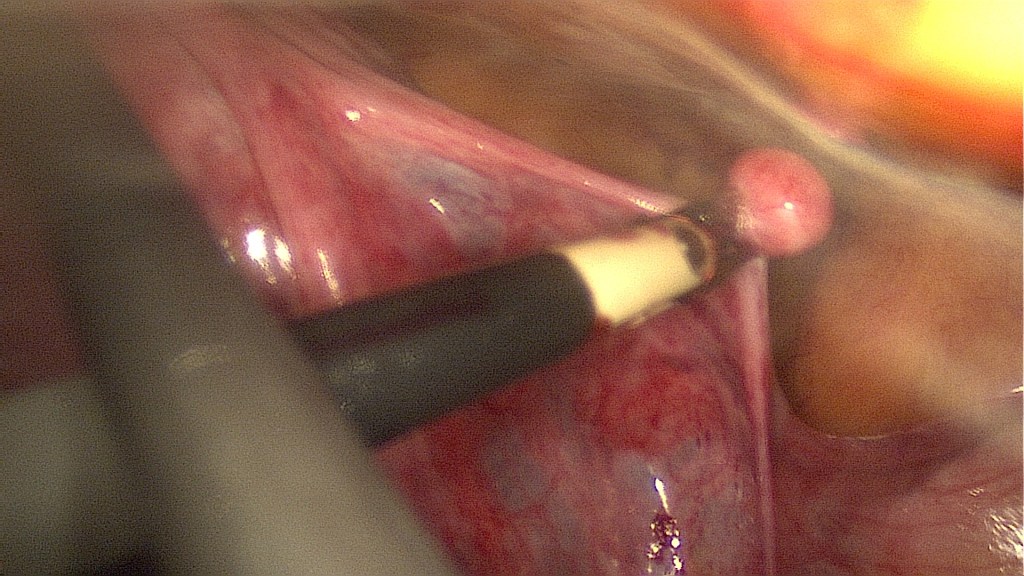
Bipolar coagulation of the pedicle. 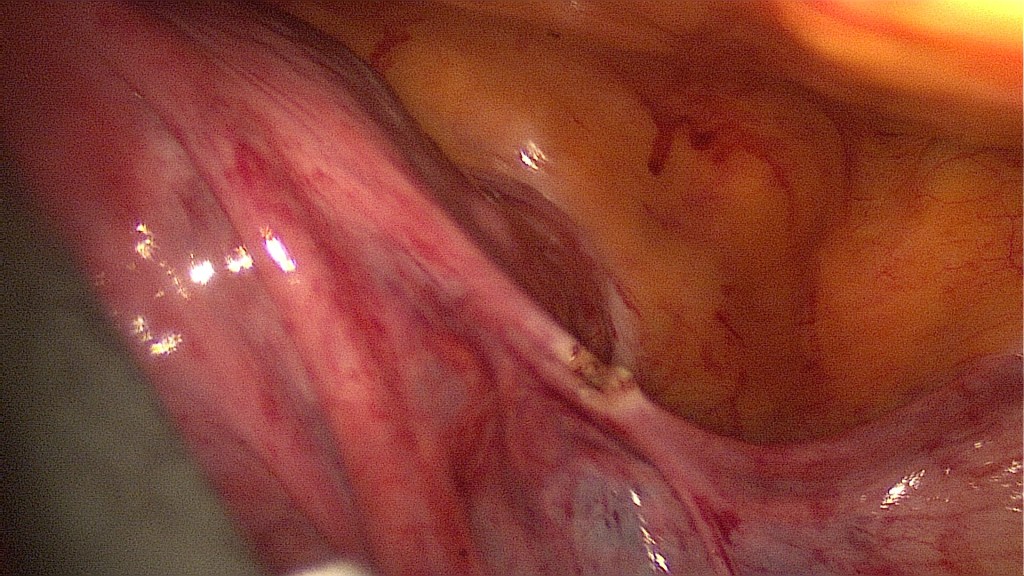
Easy excision of a myoma on the right round ligament. 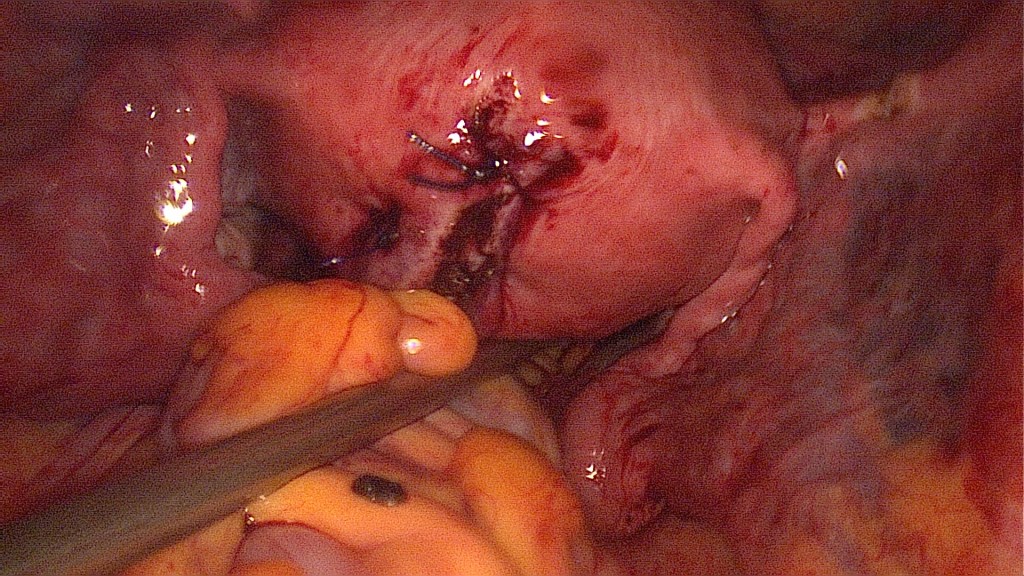
All four clips are easily removed. The total time the clips were used is being documented. 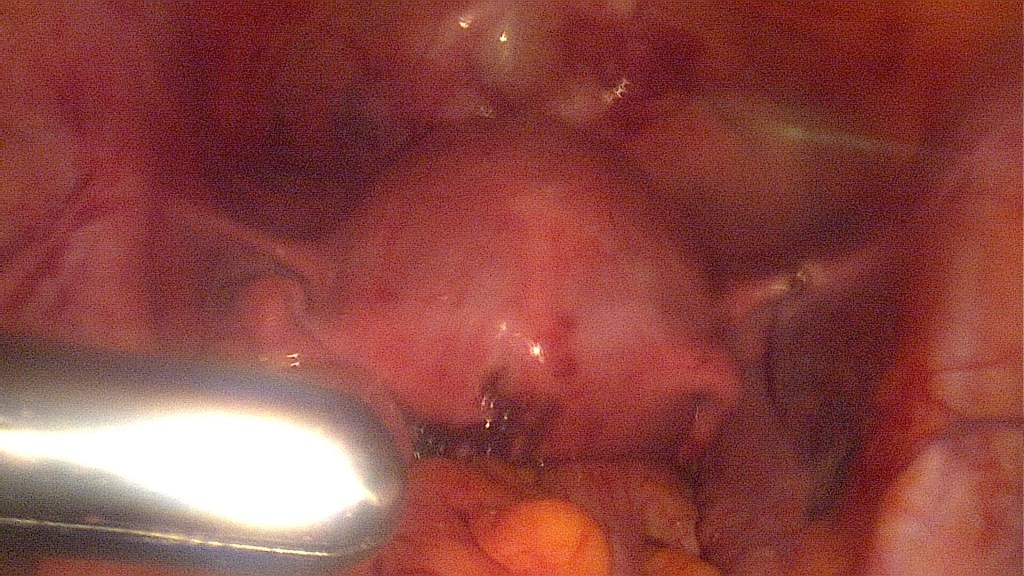
In-bag morcellation of the fibroid has been completed, a thorough check for remains has been done, then irrigation and suction ensures a clear surgical situs. 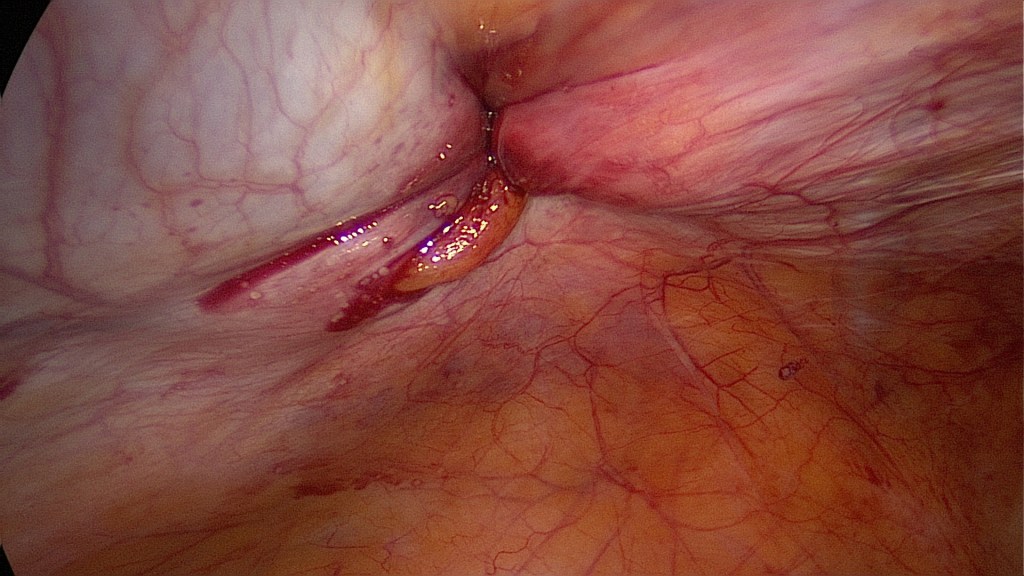
Suturing of the rectus fascia should be done in order to prevent herniation in the site of the morcellator (12mm). Here we performed endoscopic suturing of the fascia and the parietal peritoneum. 
Placement of a drainage and removal of the trocars under direct visualization.
- If necessary, a drainage can be placed at this point.
- Removal of instruments and trocars under direct visualization.
- Suturing of the fascia (facultative by trocars <11mm) and of the skin.
- Removal of bladder catheter.
Contraindications
- Patient not fit for surgery.
- Patient doesn’t have plans for future pregnancies.
- Absence of symptoms.
Complications
- Injury of nearby organs (ureter, bladder, bowel).
- Bleeding.
- Thromboembolism.
- Infection.
Postoperative Management
- Removal of drainage (if any) on 1st postoperative day.
- Routine blood test on 1st postoperative day (Hemoglobin).
- Early patient discharge (usually 2-3 days).
- Venous thromboembolism prophylaxis with low molecular weight heparin for 7 days.
- Contraception for the following 3 months.
- In case of pregnancy, every patient is given a written recommendation from the operating surgeon concerning the future mode of delivery.
Bibliography
- Rakotomahenina, H., Rajaonarison, J., Wong, L., & Brun, J. L. (2017). Myomectomy: technique and current indications. Minerva ginecologica, 69(4), 357–369. https://doi.org/10.23736/S0026-4784.17.04073-4.
- Hickman, L. C., Kotlyar, A., Shue, S., & Falcone, T. (2016). Hemostatic Techniques for Myomectomy: An Evidence-Based Approach. Journal of minimally invasive gynecology, 23(4), 497–504. https://doi.org/10.1016/j.jmig.2016.01.026.
