
Indication
Uterine/cervical prolapse.
Advantages
- Οffers easier and safer onco-preventive adnexectomy at the time of vaginal surgery.
- Creates a better anatomical correction of the prolapse in comparison to the sacrospinous ligament fixation.
- May be less risky than conventional vaginal uterosacral ligament suspension since all structures are better visualized.
- May be a better option than conventional vaginal surgery in the presence of intraperitoneal adhesions.
- As a hysteropexy, it can be a viable option for younger women with advanced prolapse wishing fertility preservation.
- Less pain and no visible scars in comparison to conventional laparoscopy.
Disadvantages
- Requires special equipment and more surgical instruments than conventional vaginal surgery.
- In comparison to its laparoscopic alternative, there is no visualization of the intraperitoneal end-result, meaning that ureteral kinking or small bowel entrapment could still occur.
- May be more time-consuming than conventional sacrospinous ligament fixation.
Technique
First perform the vaginal hysterectomy. In patients with need for uterus preservation, the peritoneal window should be opened behind the cervix (posterior colpotomy inside the cul-de-sac). 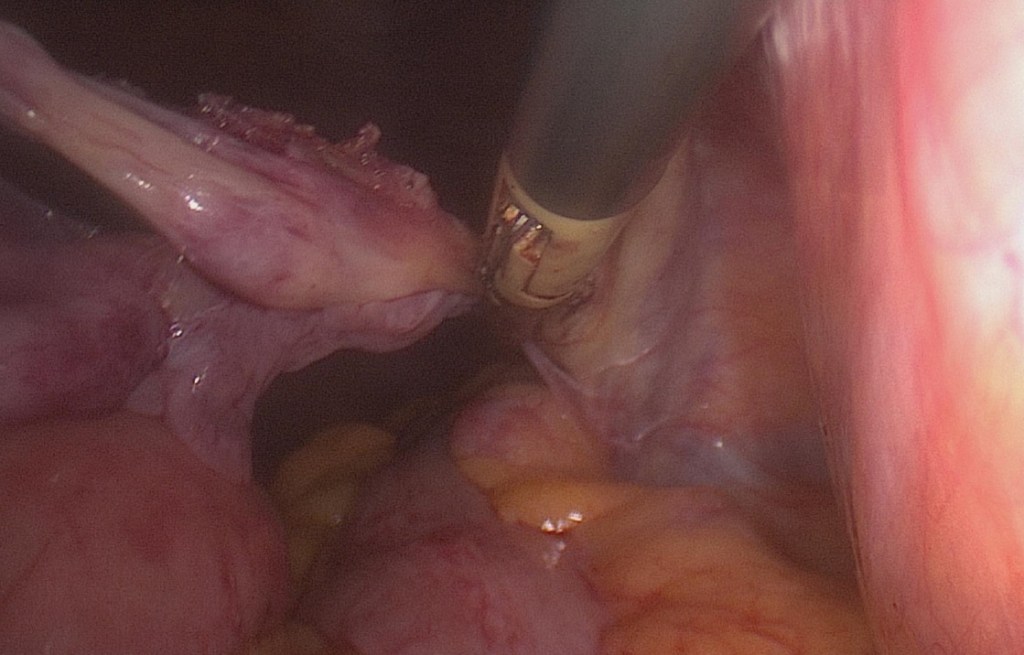
Insert your preferred transvaginal access platform (e.g. GelPOINT V-Path®) and insufflate at 12cmH20. First perform the onco-preventive adnexectomy (or salpingectomy for younger women). 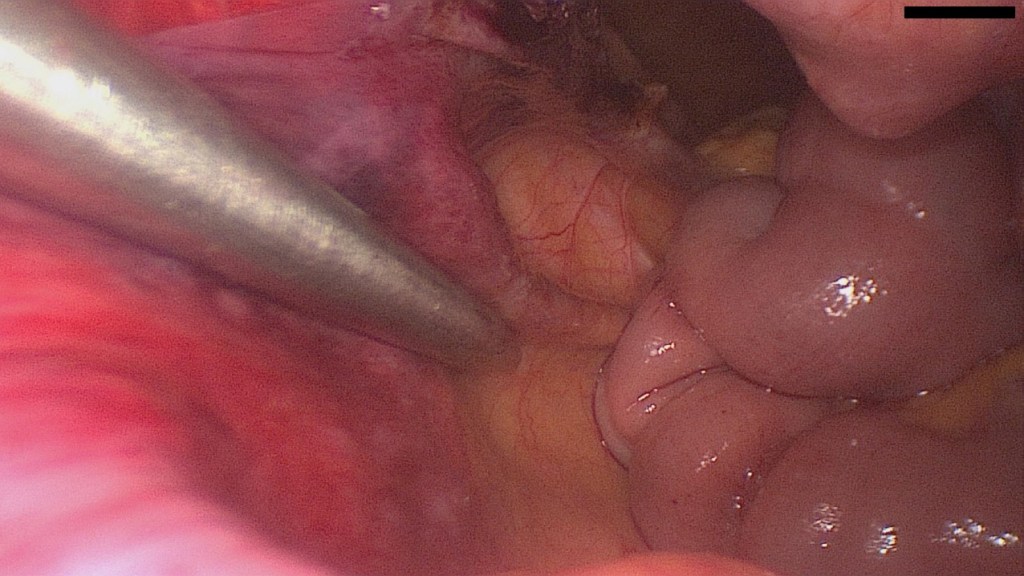
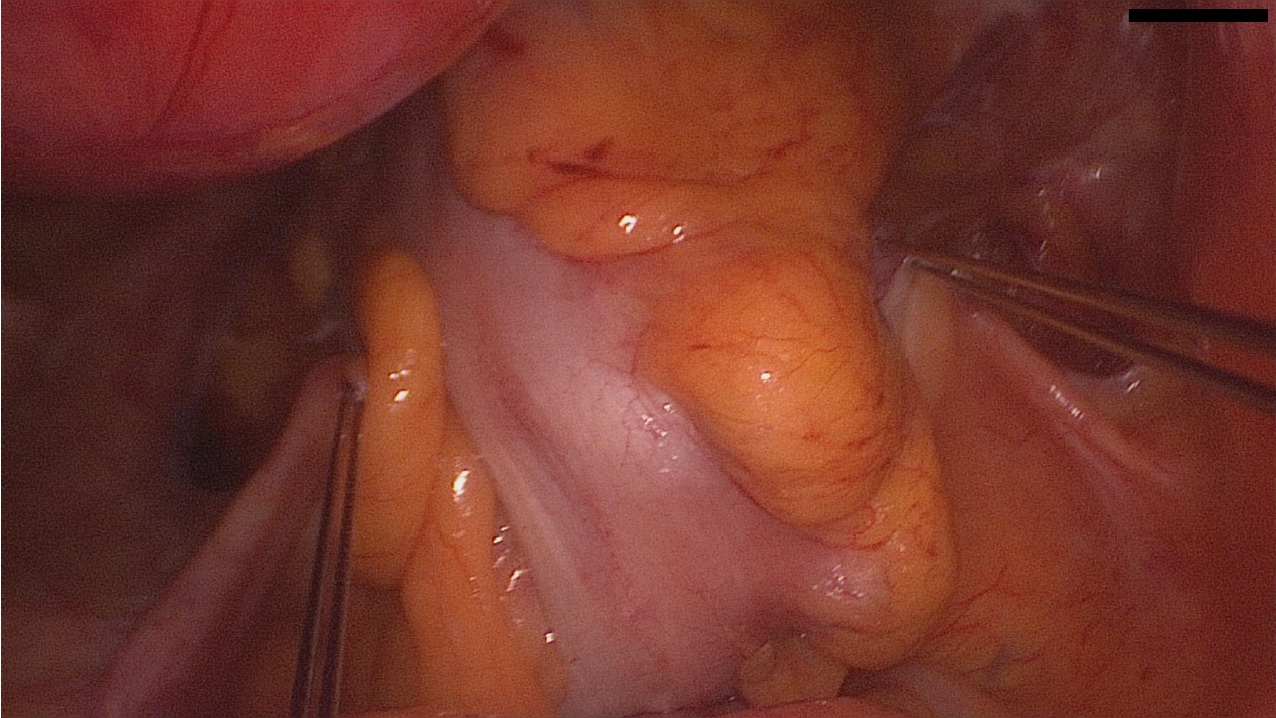
Place the patient in a slight Trendelenburg position to aid with visualization. Visualize the ureters on each side. 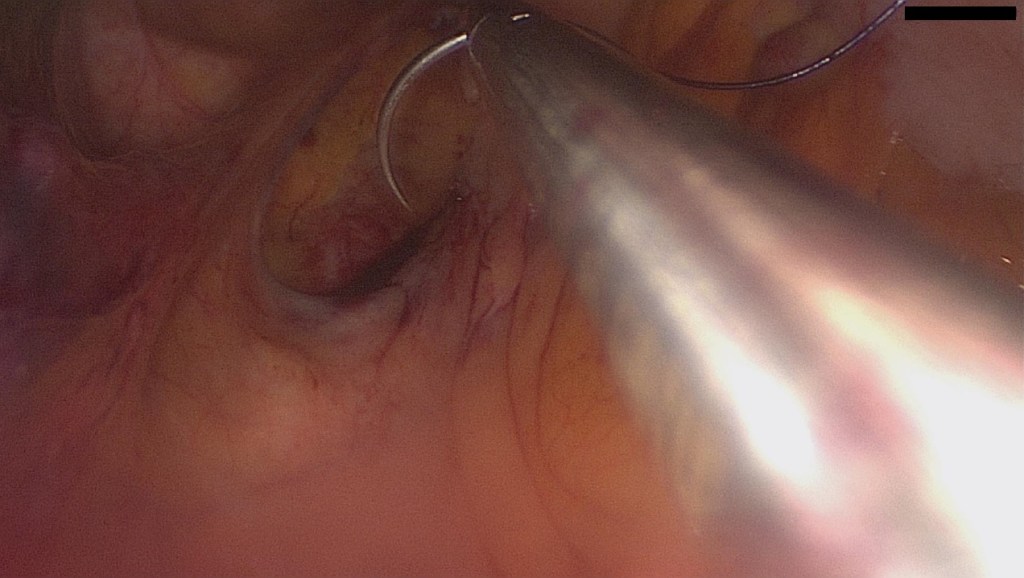
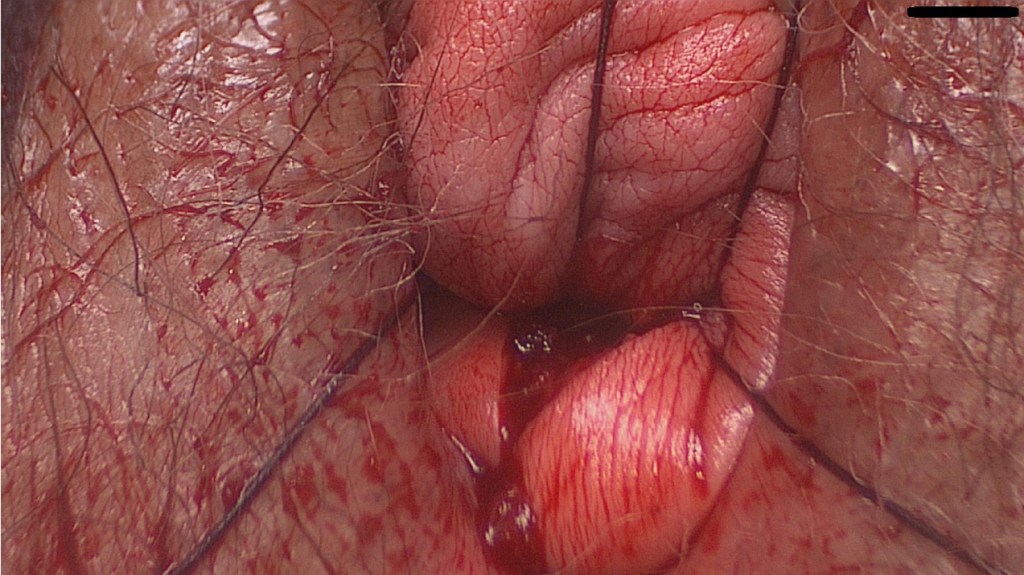
After identifying the uterosacral ligaments on each side, we prefer to open a small peritoneal window. This facilitates distancing from the ipsilateral ureter and may reduce ureteral kinking. Then we take a good grip of the uterosacral ligament, passing the suture twice and slightly pull downwards to check its strength. We use PDS 0 sutures, since absorbable sutures have been shown to not be inferior to non-absorbable. 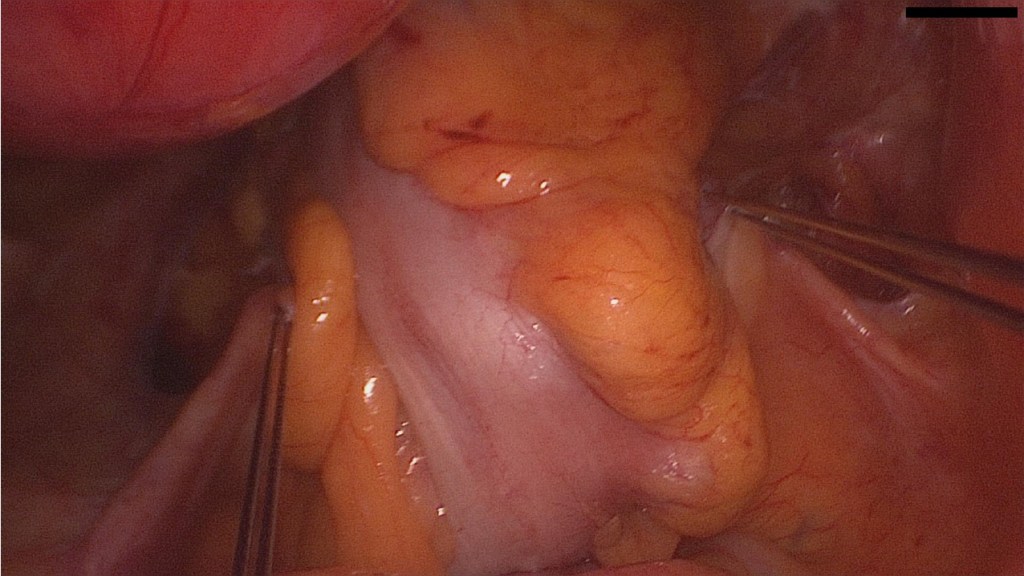
Both sutures have been passed, right and left. The vNOTES platform is removed and these are then passed through the full thickness of the posterior wall of the vaginal cuff. After completion of the surgery (anterior/posterior colporrhaphy if needed, traditional closure of the vaginal cuff) and with the patient in Trendelenburg position (to avoid entrapment of the small bowel) we tie the sutures and thus elevate the vagina.
Contraindications
- Extensive previous surgery of the pelvis – e.g. endometriosis with obliteration of the pouch of Douglas or similar.
- Conservative methods (e.g. pelvic floor training, pessary) have not been considered with the patient.
Complications
- There is a risk of recurrence, which however seems to be lower than the risk of recurrence for sacrospinous ligament fixation. Like in most pelvic organ prolapse surgeries, the highest risk of recurrence may be in the first 2 years after surgery.
- Postoperative manifestation or worsening of urinary stress incontinence.
- Ureteral kinking and hydronephrosis. This complication has been reported in as high as 11% of conventional vaginal uterosacral ligament suspensions. With vNOTES this rate may be significantly lower since the ureter is visualized and a peritoneal window may be made. In case of postoperative hydronephrosis and since the suture has only been passed through the posterior vaginal wall, cutting the ipsilateral PDS suture without anesthesia is feasible, leading to immediate alleviation of the symptoms without danger of dehiscence of the vaginal cuff.
- Urinary retention is possible, when injury of the hypogastric nerves has occurred.
Postoperative Management
- Nephrosonography on the same day (exclude ureter kinking or injury).
- Thromboembolism prophylaxis with LMWH for 7 days (avoid thrombosis – most thromboembolic events occur within the first 7 days).
- Bladder catheter for up to 24h if combined with anterior colporrhaphy (may facilitate healing of the subvesical tissue).
- Evaluation of residual urine volume before discharge (exclude hypogastric nerve injury). See how to sonographically determine the postvoid residual bladder volume here.
Bibliography
- Greene, K.A., Wyman, A.M., Tamhane, N. et al. Adnexal surgery at the time of hysterectomy in women 65 years and older undergoing hysterectomy for prolapse: do practice trends differ by route of surgery?. Int Urogynecol J 32, 2185–2193 (2021). https://doi.org/10.1007/s00192-020-04663-0
- Kowalski, J.T., Genadry, R., Ten Eyck, P. et al. A randomized controlled trial of permanent vs absorbable suture for uterosacral ligament suspension. Int Urogynecol J 32, 785–790 (2021). https://doi.org/10.1007/s00192-020-04244-1
- Husby, K.R., Larsen, M.D., Lose, G. et al. Surgical repair of vaginal vault prolapse; a comparison between ipsilateral uterosacral ligament suspension and sacrospinous ligament fixation—a nationwide cohort study. Int Urogynecol J 32, 1441–1449 (2021). https://doi.org/10.1007/s00192-020-04515-x
- Roos, E.J., Schuit, E. Timing of recurrence after surgery in pelvic organ prolapse. Int Urogynecol J 32, 2169–2176 (2021). https://doi.org/10.1007/s00192-021-04754-6
- Lowenstein, L., Baekelandt, J., Paz, Y., Lauterbach, R., & Matanes, E. (2019). Transvaginal Natural Orifice Transluminal Endoscopic Hysterectomy and Apical Suspension of the Vaginal Cuff to the Uterosacral Ligament. Journal of minimally invasive gynecology, 26(6), 1015. https://doi.org/10.1016/j.jmig.2019.04.007
- Dubuisson, J., Claver, M., & Constantin, F. (2021). Suspension haute du dôme vaginal aux ligaments utérosacrés par Transvaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) (avec vidéo) [Transvaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) for high uterosacral ligament suspension of the vaginal cuff (with video)]. Gynecologie, obstetrique, fertilite & senologie, S2468-7189(21)00049-0. Advance online publication. https://doi.org/10.1016/j.gofs.2021.02.009
- Lowenstein, L., Matanes, E., Lauterbach, R., Mor, O., Burke, Y. Z., Weiner, Z., & Baekelandt, J. (2021). Feasibility and Learning Curve of Transvaginal Natural Orifice Transluminal Endoscopic Surgery for Hysterectomy and Uterosacral Ligament Suspension in Apical Compartment Prolapse. Female pelvic medicine & reconstructive surgery, 27(1), e171–e176. https://doi.org/10.1097/SPV.0000000000000875
- Lu, Z., Chen, Y., Wang, X., Li, J., Hua, K., & Hu, C. (2021). Transvaginal natural orifice transluminal endoscopic surgery for uterosacral ligament suspension: pilot study of 35 cases of severe pelvic organ prolapse. BMC surgery, 21(1), 286. https://doi.org/10.1186/s12893-021-01280-6
- Aharoni, S., Matanes, E., Lauterbach, R., Mor, O., Weiner, Z., & Lowenstein, L. (2021). Transvaginal natural orifice transluminal endoscopic versus conventional vaginal hysterectomy with uterosacral ligament suspension for apical compartment prolapse. European journal of obstetrics, gynecology, and reproductive biology, 260, 203–207. https://doi.org/10.1016/j.ejogrb.2021.03.040
