
1. Abdominal and thoracic situs
The fetal echocardiography should commence with the identification of the abdominal situs and the fetal position. Normal visceral situs or situs solitus is defined by presence of the stomach, the heart and the descending aorta on the left side, while the inferior vena cava is located on the right side.
Anomalies: situs ambiguous (heterotaxy), situs inversus.
2. Heart occupies 1/3 to 1/2 of thoracic area
The cardiothoracic (C/T) circumference measured during diastole is fairly constant throughout gestation, ranging between 0.38 at 11 weeks, increasing slightly up to 0.5 at term in normal fetuses.
Anomalies: cardiomegaly, lethal skeletal dysplasia, severe pulmonary hypoplasia.
3. Position of the heart on the left, apex points to left by 45◦ ± 20◦
The imaginary line between sternum and spine should divide the heart leaving the bigger part on the left side and also the apex points towards the left (levocardia).
Anomalies: mesocardia, dextrocardia (dextroversion or dextroposition), excessive levocardia, levoposition.
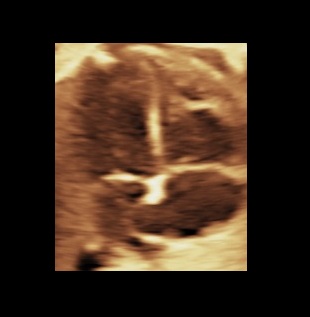
4. Four anatomically distinct chambers present
Two atria (approx. equal in size) and two ventricles (approx. equal in size). The anatomic left atrium has a hook shaped appendage, while the anatomic right atrium has a broad pyramidal shaped appendage. Also, the left atrium receives the four pulmonary veins, two of them – the inferior ones – can be identified in the four chamber view. The anatomic left ventricle forms the cardiac apex, while the anatomic right ventricle contains the moderator band.
Anomalies: atrioventricular valve regurgitation, Ebstein anomaly, cardiac anomalies that may show a single ventricle, heterotaxy, congenitally corrected transposition of the great vessels, total or partial anomalous pulmonary venous return.
5. Normal cardiac crux
In normal cases the septum primum can be identified near the crux. The tricuspid valve leaflet inserts on ventricular septum closer to cardiac apex than does mitral valve (differential offsetting of the AV-valves). Both valves open and move freely. Also the ventricular wall has to be in contact with the crux.
Anomalies: atrial (I), ventricular (inlet) or atrioventricular septal defect.
6. Foramen ovale leaflet in left atrium
Flow from right to left on color mode.
Anomalies: left-to-right shunting across the foramen ovale.
7. Ventricular septum intact
From apex to crux. Note that the four chamber view can detect only inlet-type and some of the muscular-type septal defects.
Anomalies: ventricular septal defect.
8. Cardiac wall
No hypertrophy of the ventricular wall, no pericardial effusion.
Anomalies: hypertrophic cardiomyopathy, pericardial effusion.
9. Regular cardiac rhythm
On a live examination the cardiac rhythm is identifiable and should be documented.
Anomalies: arrhythmia.


MB: moderator band, RV: right ventricle, TV: tricuspid valve, RA: right atrium, Fo: foramen ovale, SP: septum primum, PV: inferior pulmonary veins, Ao: aorta, LA: left atrium, MV: mitral valve, LV: left ventricle, VS: ventricular septum.
Bibliography
- Carvalho, J. , Allan, L. , Chaoui, R. , Copel, J. , DeVore, G. , Hecher, K. , Lee, W. , Munoz, H. , Paladini, D. , Tutschek, B. and Yagel, S. (2013), ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol, 41: 348-359. doi:10.1002/uog.12403
- Abuhamad, Alfred, and Rabih Chaoui. A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts. 2nd ed., Wolters Kluwer, 2010.
- Paladini, D., Chita, S. K., & Allan, L. D. (1990). Prenatal measurement of cardiothoracic ratio in evaluation of heart disease. Archives of Disease in Childhood, 65(1 Spec No), 20–23.
