

Indication
Tubal ectopic pregnancy.
Technique
The following technique refers to tubal ectopic pregnancy located in the ampulla (most common type).
Step-wise approach with intraoperative photos and video of the procedure ensues:
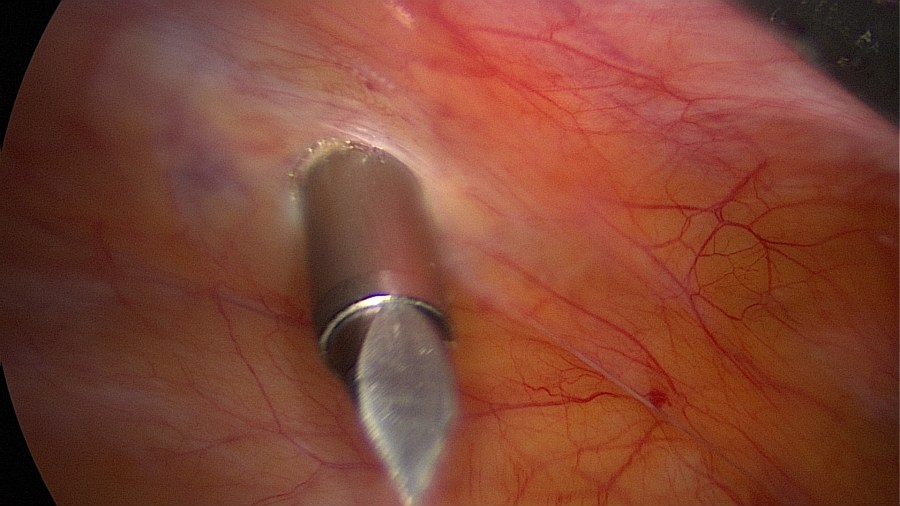
Gain intraperitoneal access and ensure adequate visualization of the small pelvis. 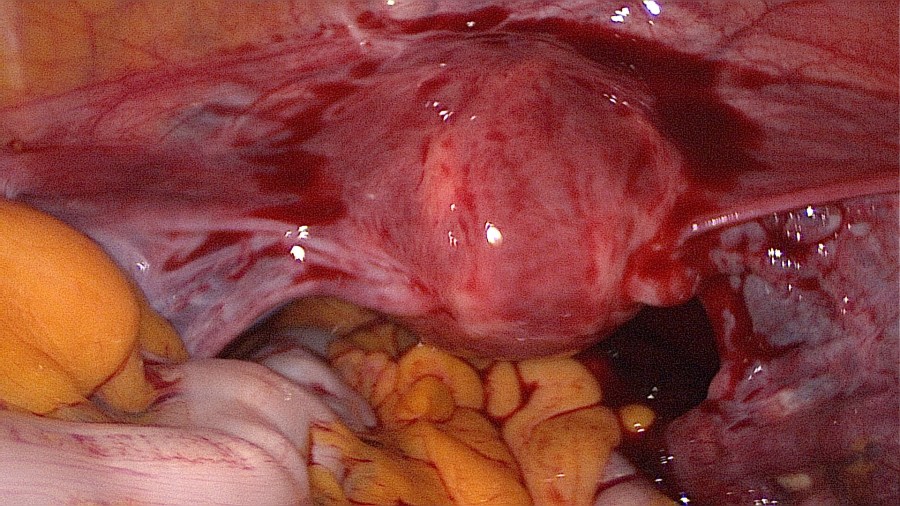
Inspect the organs in the small pelvis thoroughly and drain any blood that may have accumulated. 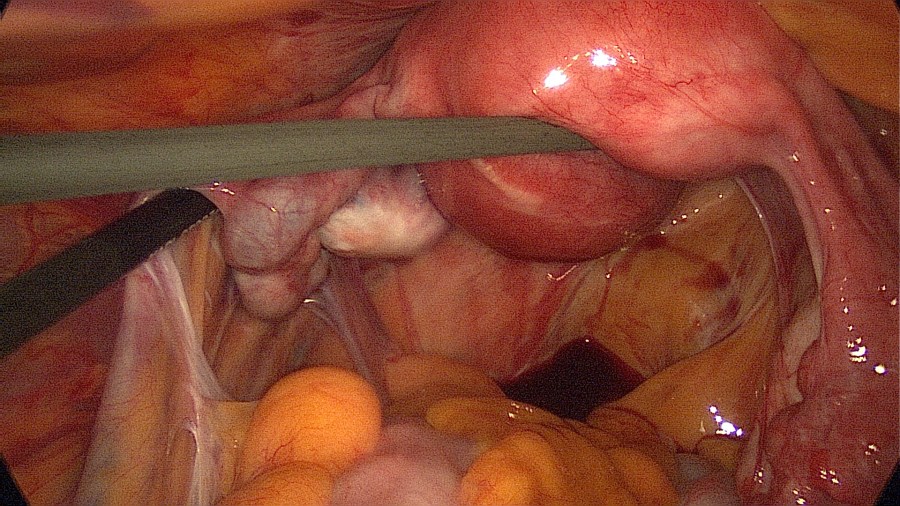
Know your situs: in this case there are pelvic adhesions after pelvic inflammatory disease. 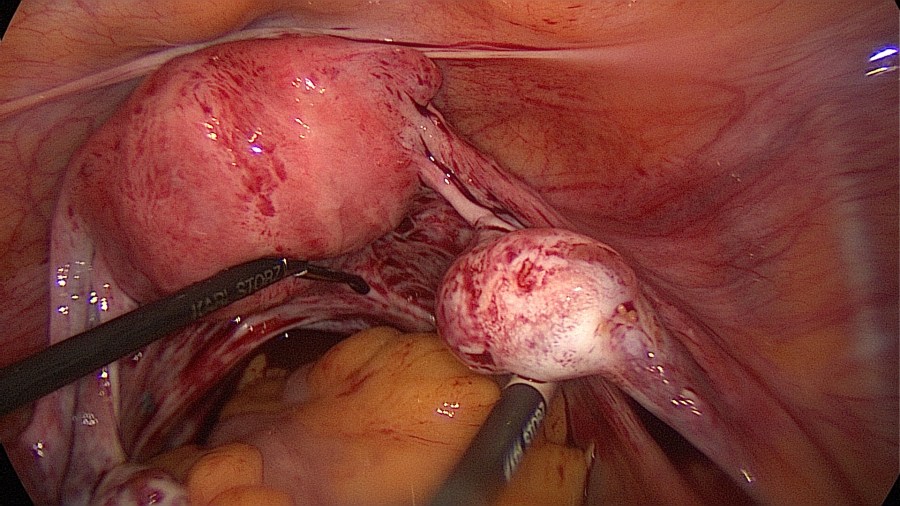
Know your situs: Here the right tube is missing after a previous salpingectomy for ectopic pregnancy. Treating the ectopic pregnancy on the left side (not seen here) has got to be delicate. 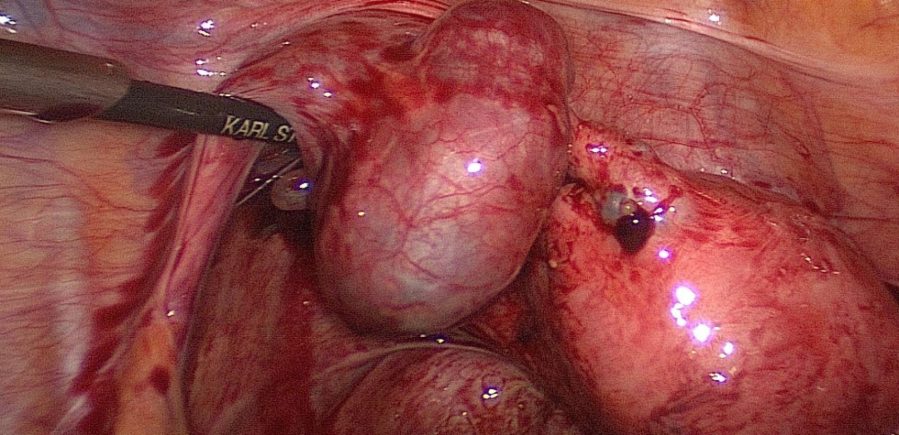
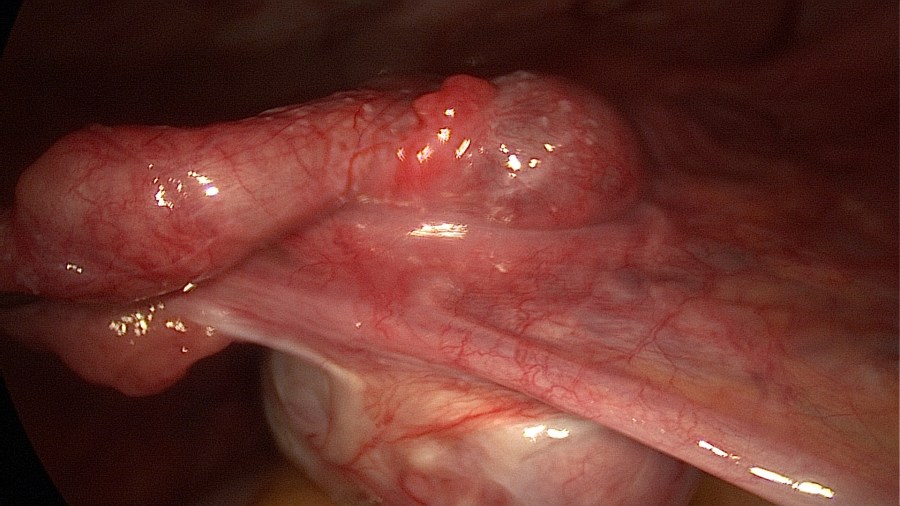
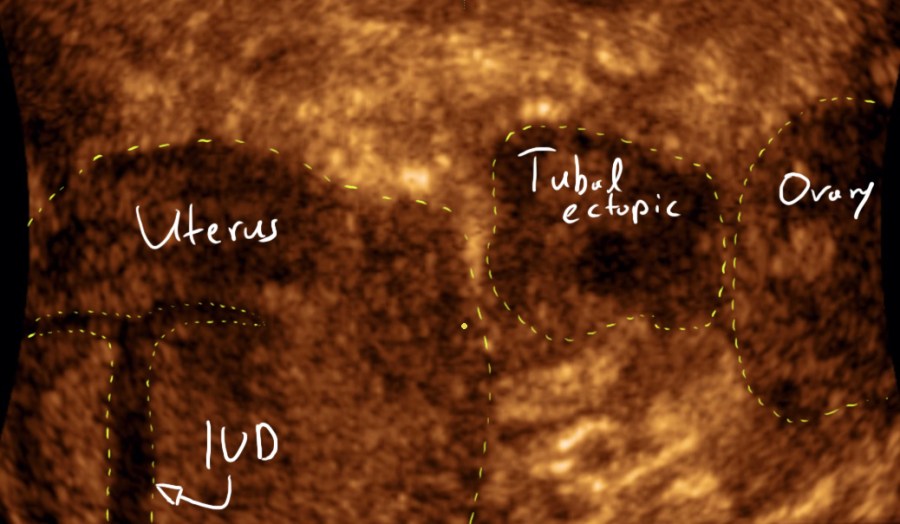
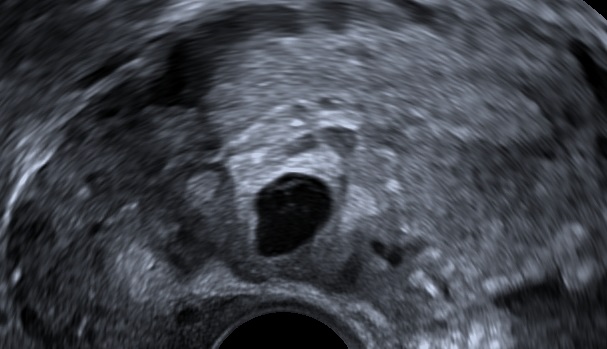
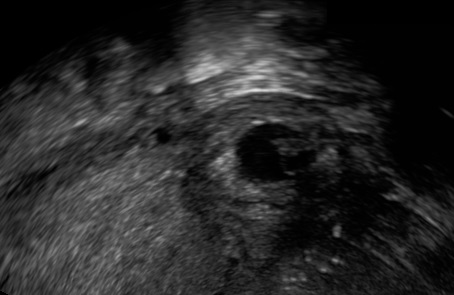
Visualize the ectopic pregnancy. 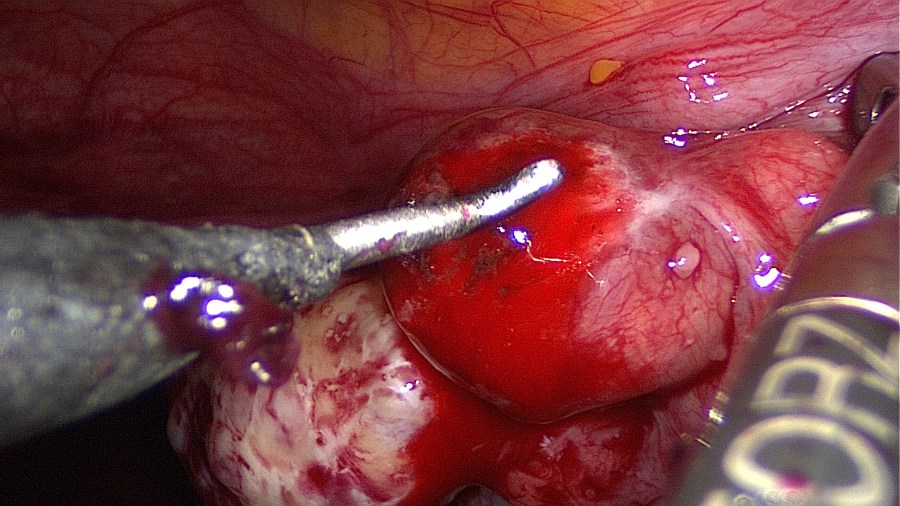
Linear salpingotomy: open the tube directly over the tubal pregnancy with a straight incision made with a monopolar needle (Taran, F-A et al., 2015). 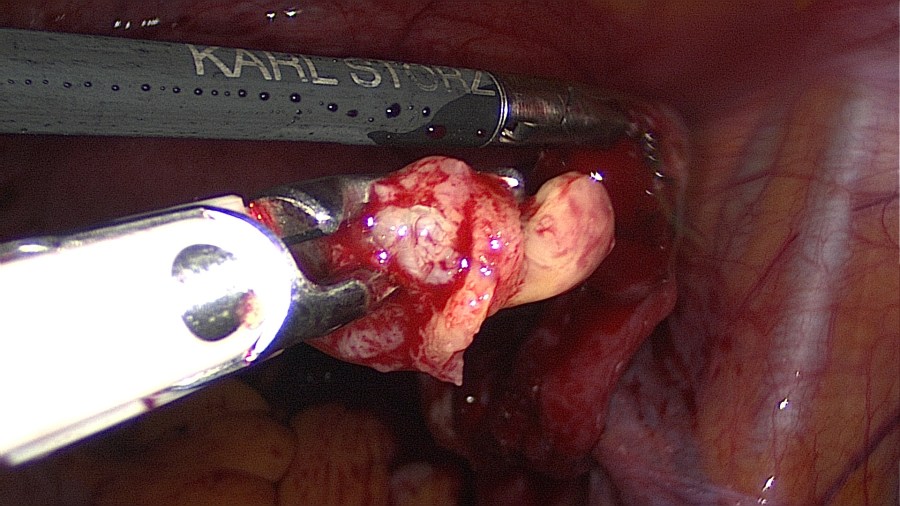
Grasp the contents with an atraumatic grasper and expell the tubal pregnancy en bloc. Failure to do so may increase risk of persistent ectopic tissue. Alternatively this may be performed with suction or aquadissection. 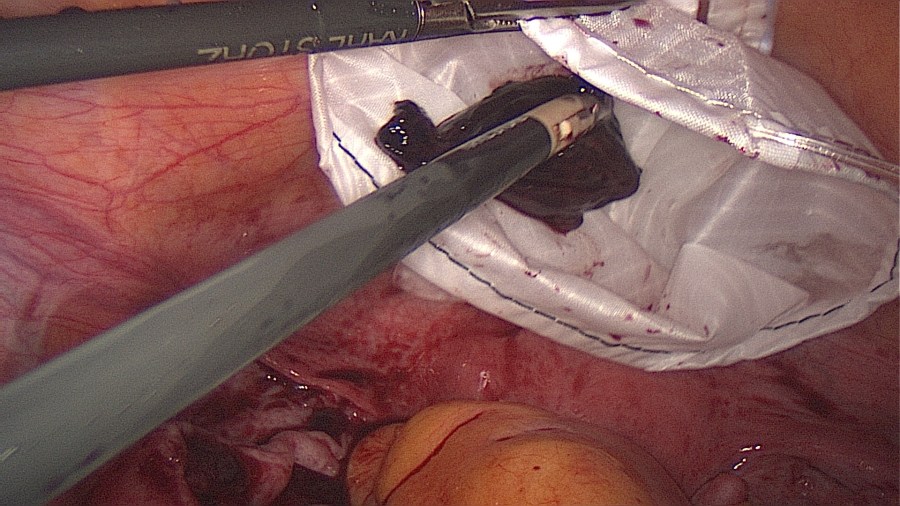
Bring the ectopic material inside a retriever bag and close it. 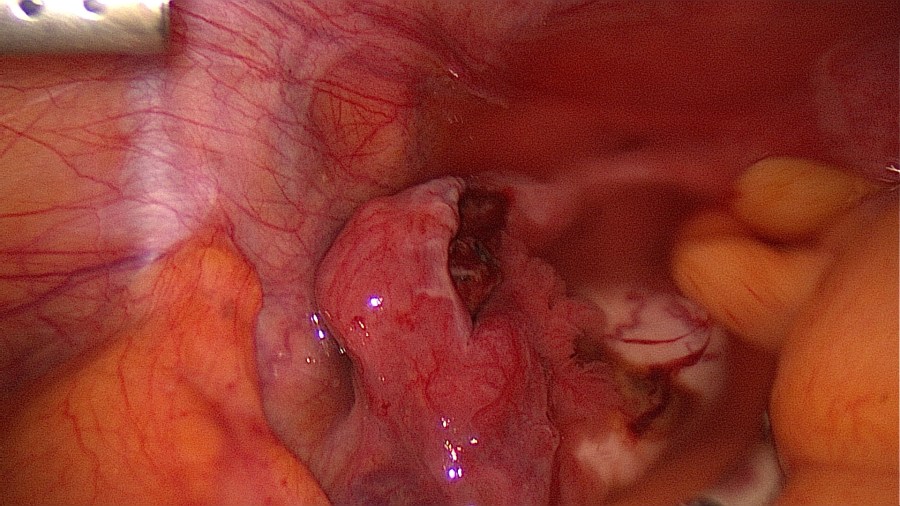
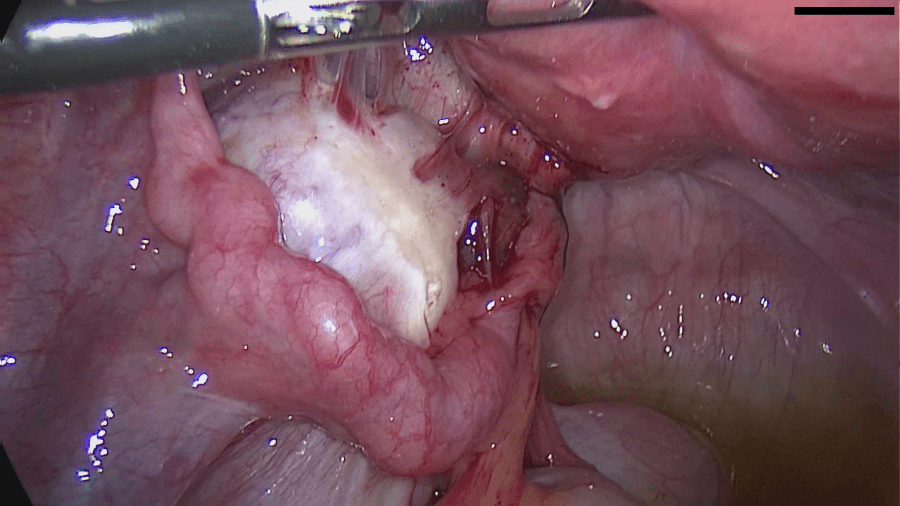
If need be, control the bleeding with tissue-sparing bipolar coagulation. In this case the tube (submerged in saline) does not require any coagulation or suturing. 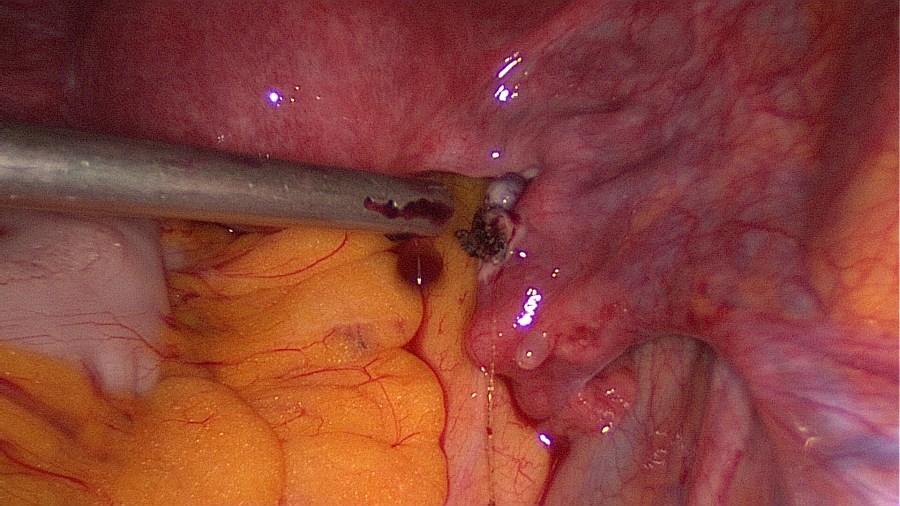
While most of the time not necessary, suturing may decrease the damage done to fallopian tube and aid in the recovery of its normal anatomy, especially in large defects (Li, L et al., 2016). In this case the right tube was sutured. 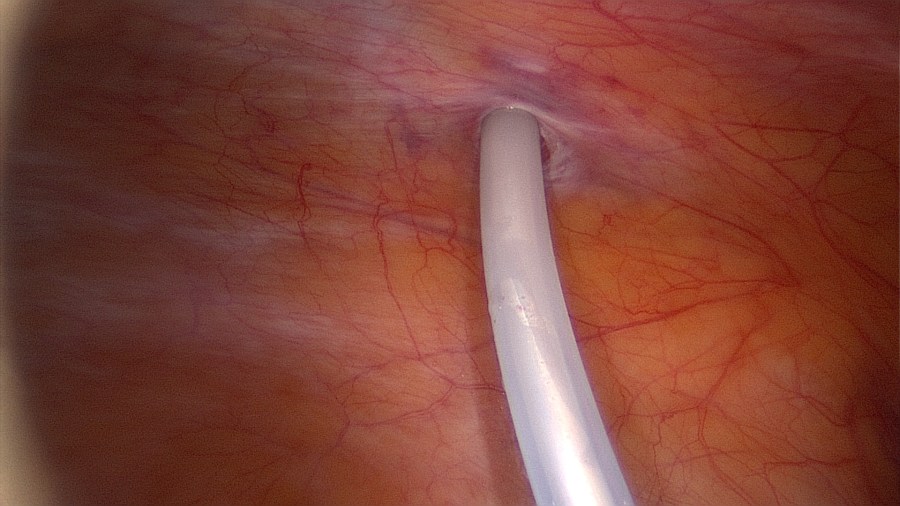
Remove the retriever bag, wash the pelvis, place a drainage (i.e. Robinson 15).
Contraindications
- Previous tubal ectopic on the same side.
- Patient wishes salpingectomy after informed consent.
Complications
- Persistent trophoblast / ectopic tissue.
- Repeat ectopic pregnancy on the same side.
- Bleeding (Moll, F et al., 2014).
Postoperative Management
- Removal of drainage on 1st postoperative day.
- Beta-hCG on 1st postoperative day.
- Thrombosis prophylaxis with low molecular weight heparin 1x s.c. 6h after surgery.
- Early discharge (1st postoperative day).
You might also find interesting other articles on ectopic pregnancy:
Bibliography
- Mol, F., van Mello, N. M., Strandell, A., Strandell, K., Jurkovic, D., Ross, J., Barnhart, K. T., Yalcinkaya, T. M., Verhoeve, H. R., Graziosi, G., Koks, C., Klinte, I., Hogström, L., Janssen, I., Kragt, H., Hoek, A., Trimbos-Kemper, T., Broekmans, F., Willemsen, W., Ankum, W. M., … European Surgery in Ectopic Pregnancy (ESEP) study group (2014). Salpingotomy versus salpingectomy in women with tubal pregnancy (ESEP study): an open-label, multicentre, randomised controlled trial. Lancet (London, England), 383(9927), 1483–1489. https://doi.org/10.1016/S0140-6736(14)60123-9
- Li, L., Wang, J. J., & Cheng, J. M. (2016). Zhonghua yi xue za zhi, 96(30), 2424–2426. https://doi.org/10.3760/cma.j.issn.0376-2491.2016.30.012
- Taran, F.-A., Kagan, K.-O., Hübner, M., Hoopmann, M., Wallwiener, D., & Brucker, S. (2015). The Diagnosis and Treatment of Ectopic Pregnancy. Dtsch Arztebl International, 112(41), 693–704. Retrieved from https://www.aerzteblatt.de/int/article.asp?id=172413
