
Indication
- Benign gynecological conditions
- Uterine fibroids causing serious symptoms (with exception of small, singular intracavitary fibroids FIGO I or II).
- High suspicion of adenomyosis uteri interna resistant to endocrine therapy.
- Dysfunctional uterine bleeding resistant to endocrine therapy or endometrial ablation.
- Gynecological malignancy
- Endometrial cancer.
- Precancerous lesions of the cervix when CIN 2/3 persists even after conization.
- Borderline ovarian tumor.
Technique
- Preoperative antibiotic prophylaxis (single shot, second generation cephalosporine).
- Patient in lithotomy position.
- Desinfection of the abdomen, thighs, vulva and vagina.
- Sterile surgical drapes.
- Urinary catheter.
- Examination under anesthesia.
- Uterine Manipulator.
- Change of surgical gloves, start of laparoscopy.

As usual in laparoscopy, inspection of the whole peritoneal cavity should be performed. 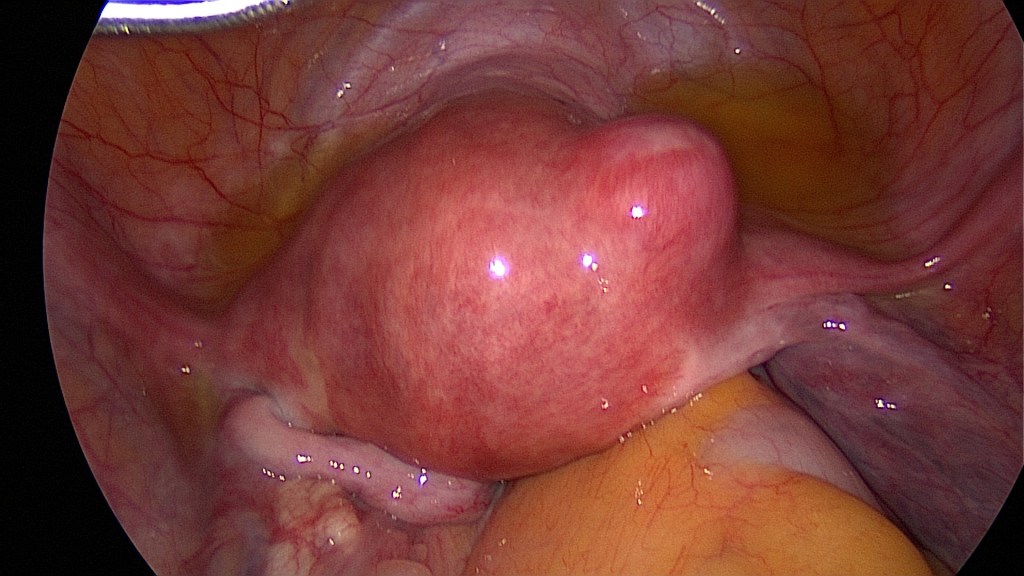
Uterine fibroids as an indication for hysterectomy. 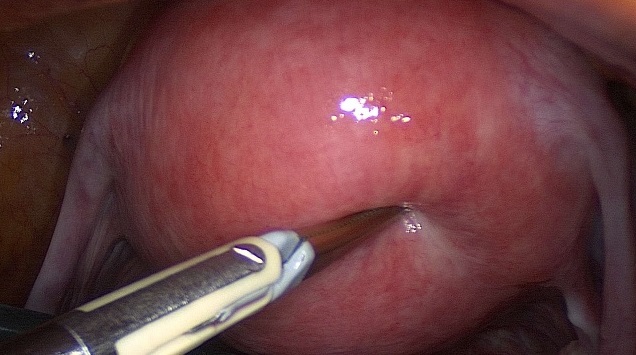
Adenomyosis uteri as an indication for hysterectomy. 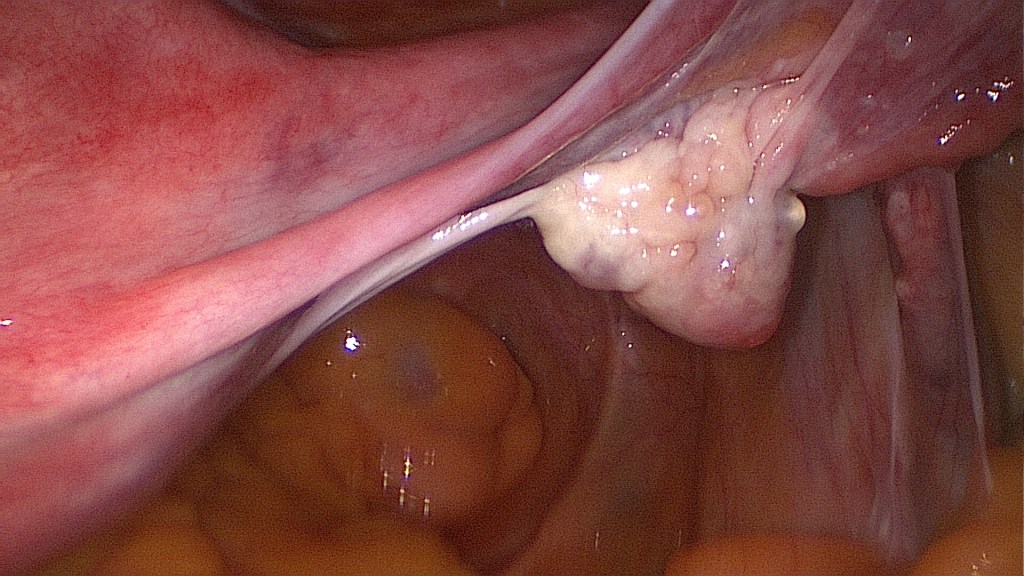
Inspection and documentation of the normal ovaries. 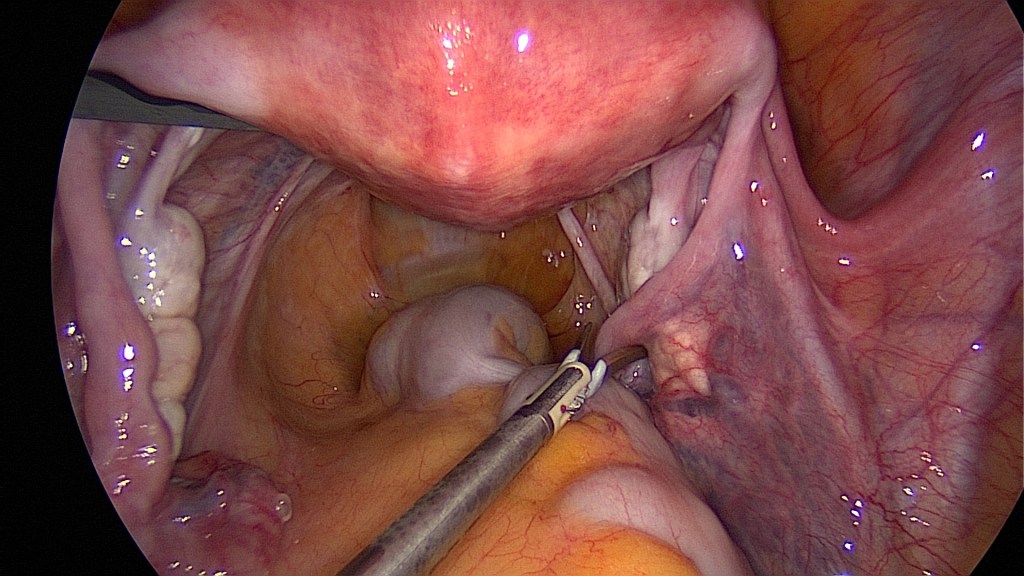
Begin with the oncoprophylactic salpingectomy. 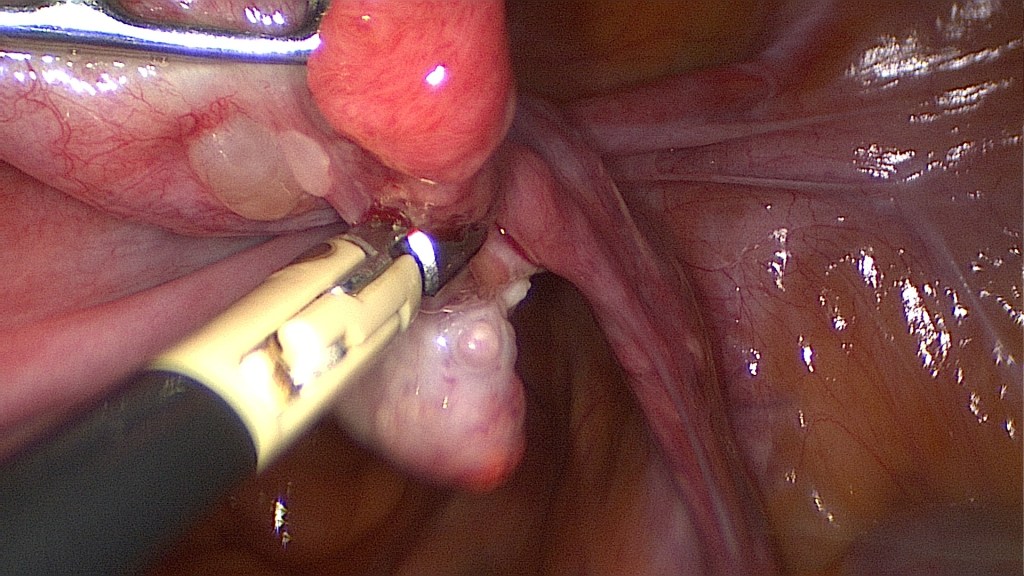
Care is to be taken in order to avoid injury of the ovarian vessels. 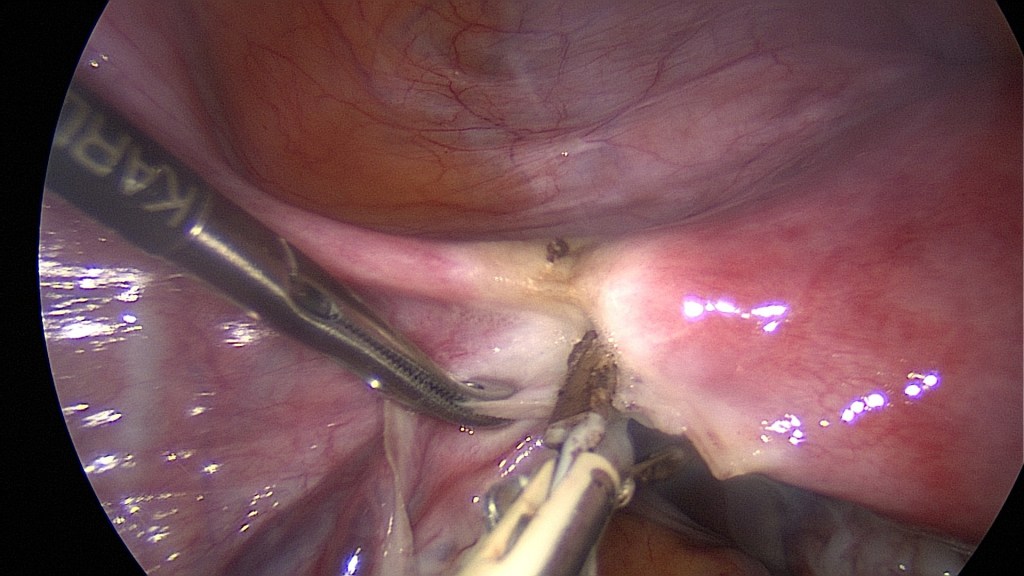
Bipolar coagulation of the round ligament (lig. rotundum) and cutting of the utero-ovarian ligament (lig. ovarii proprium). 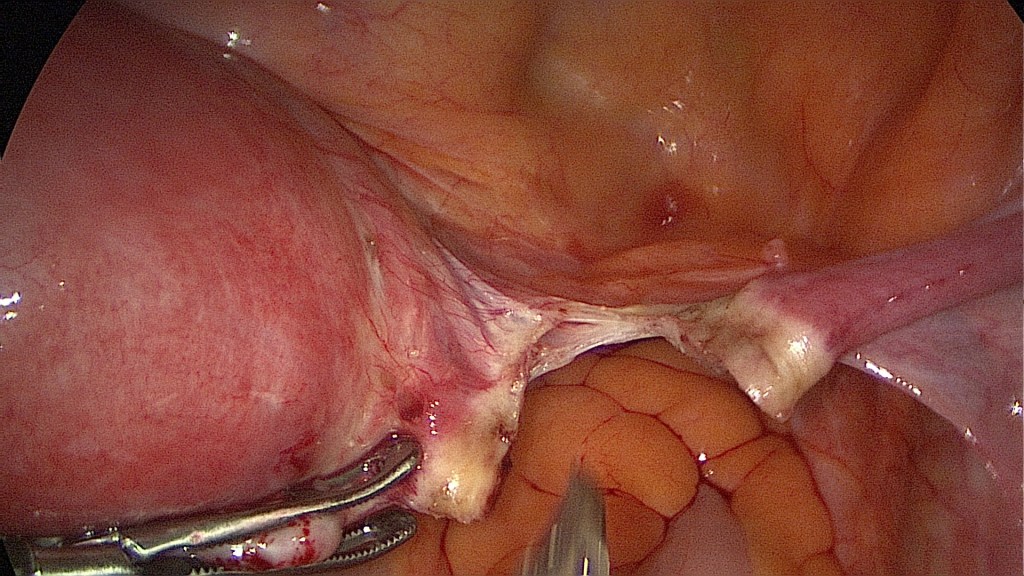
Cutting of the round ligament (lig. rotundum). 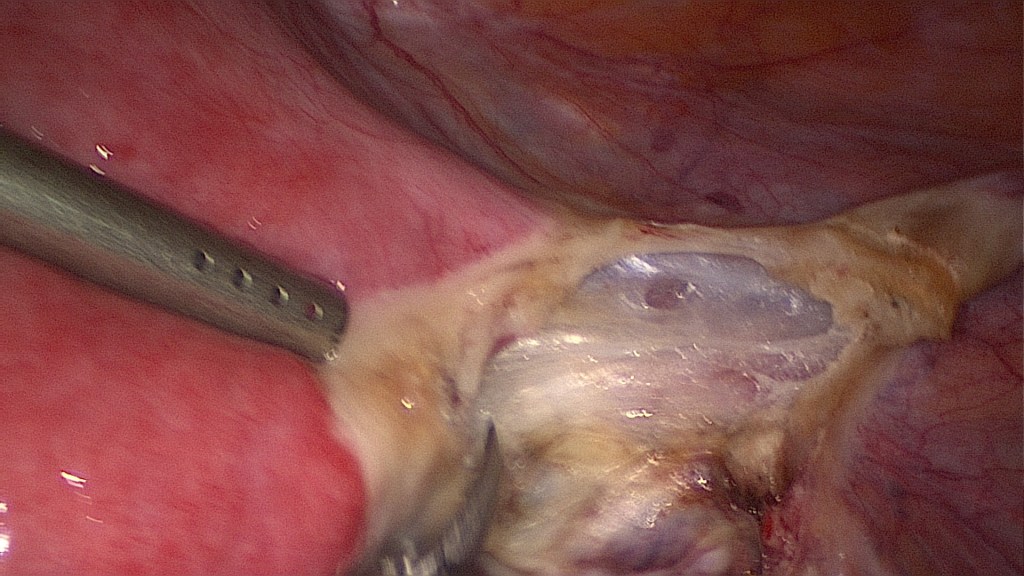
Separating the leaves of the broad ligament (lig. latum). 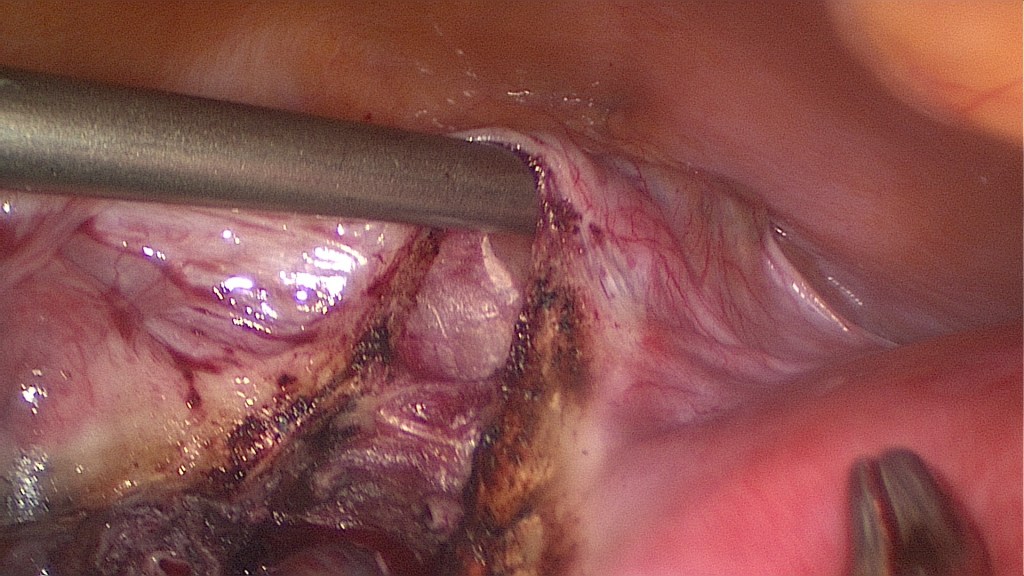
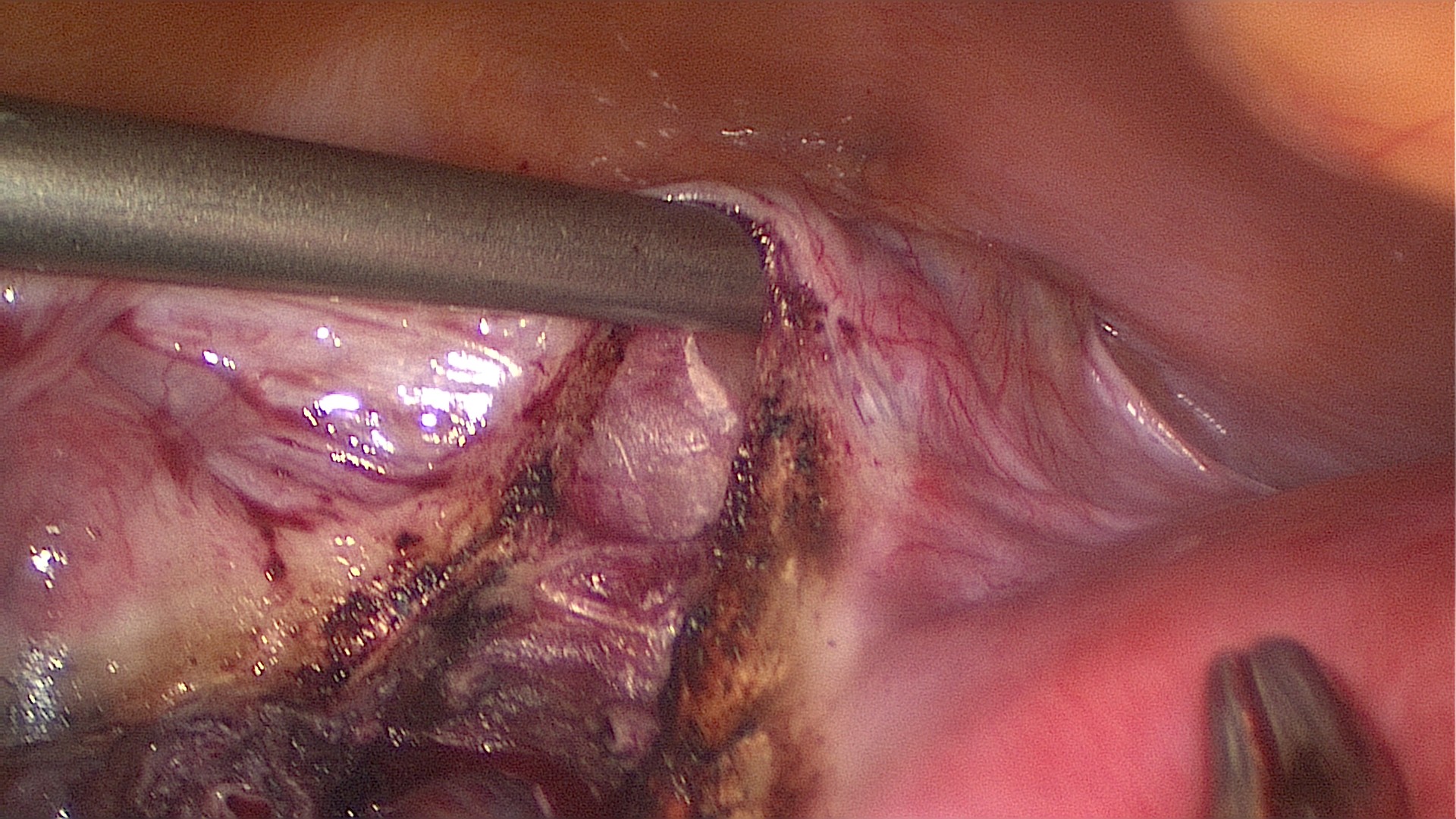
With the suction the bladder peritoneum can be elevated in order to safely open it. 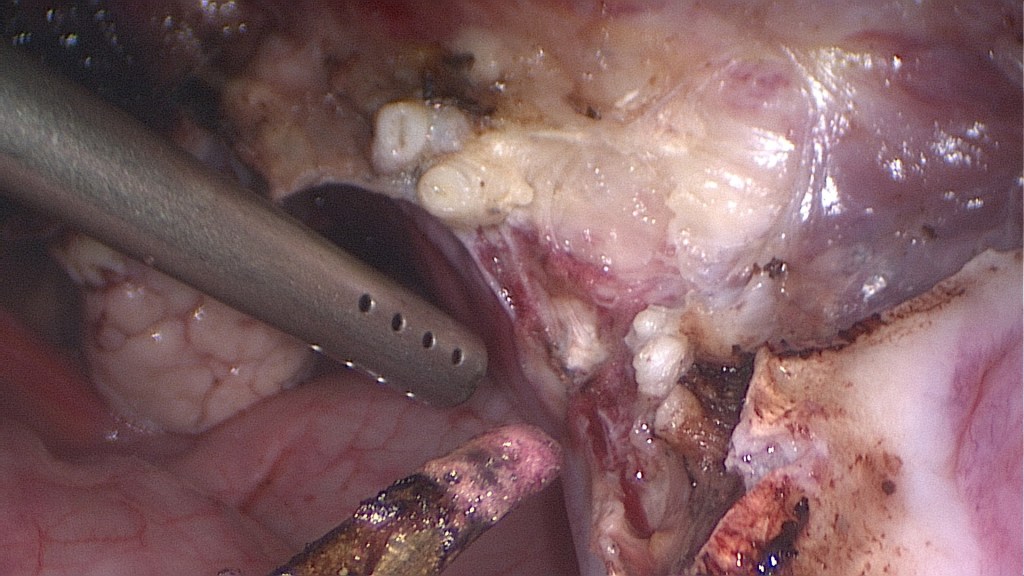
After securing the bladder the uterine vessels are coagulated and cut. Here two uterine arteries are seen, a not so rare variant. 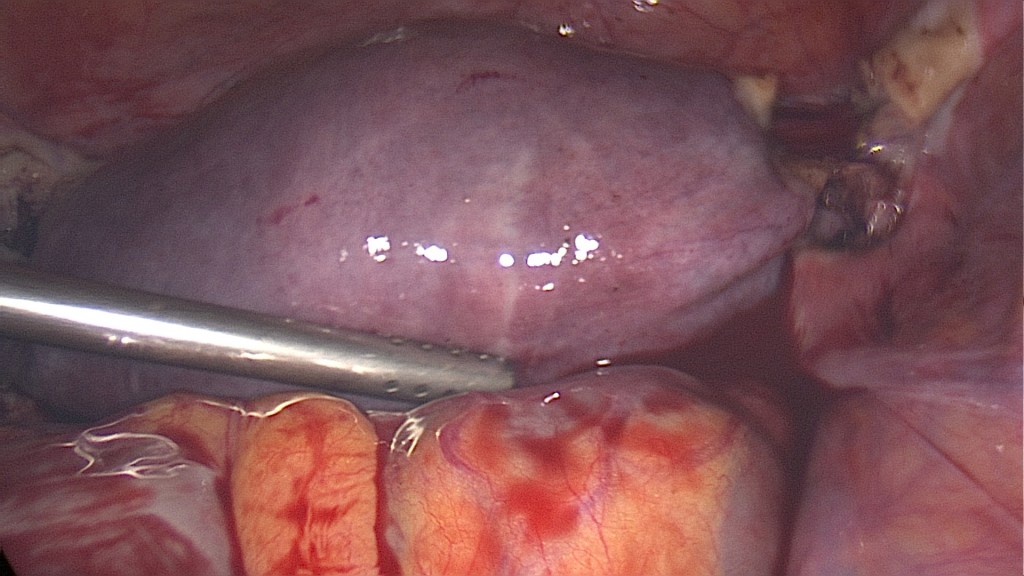
After cutting of the uterine vessels the uterus appears livid. 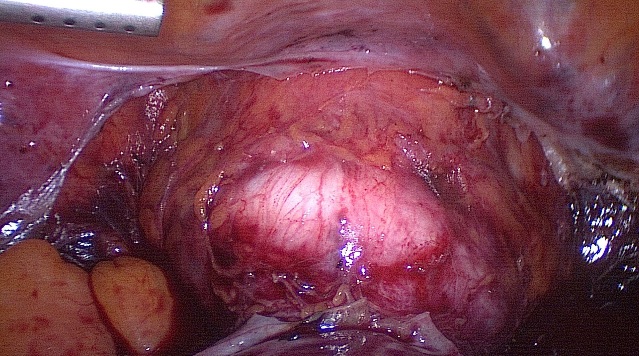
Pushing the manipulator cranially helps identify the vagina. Here the appropriate plane has been disected and the colpotomy can now be performed with monopolar cautery. 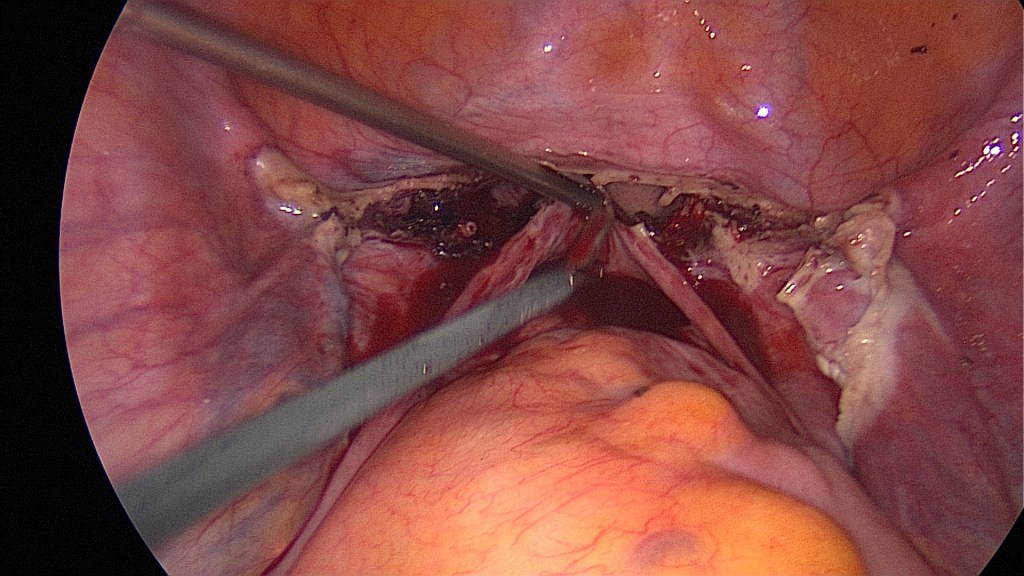
After completion of the circular colpotomy the uterus should be free and may be vaginally extracted. 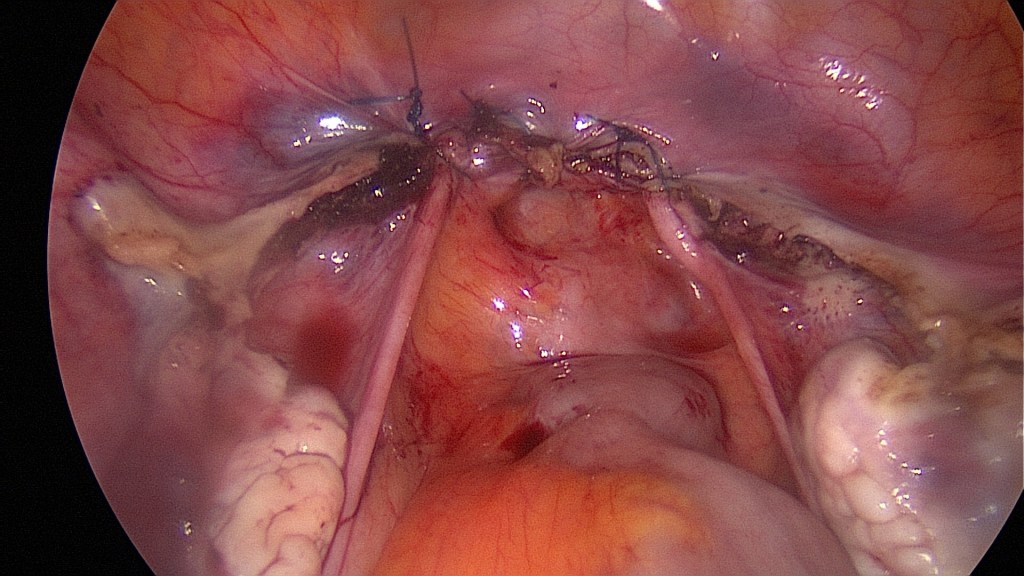
There is great variation in the suturing of the vaginal cuff (intracorporeal/extracorporeal, interrupted/continuous, with peritoneal closure/without peritoneal closure, with inclusion of the sacrouterine ligaments/without inclusion of sacrouterine ligaments). However every author tends to agree on one thing; the vaginal epithelium has to be included in the suture, otherwise vaginal bleeding would persist. Bipolar coagulation should be kept to a minimum, since it can lead to necrosis and dehiscence.
- If necessary, a drainage can be placed at this point.
- Removal of instruments and trocars under direct visualization.
- Suturing of the fascia (facultative by trocars <11mm) and of the skin.
- Removal of bladder catheter.
Contraindications
- Patient not fit for surgery.
- Patient has further plans for bearing children.
Complications
- Injury of nearby organs (ureter, bladder, bowel).
- Bleeding.
- Thromboembolism.
- Infection.
Postoperative Management
- Removal of drainage (if any) on 1st postoperative day.
- Routine blood test on 1st postoperative day (Hemoglobin).
- Early patient discharge (usually just a few days).
- Venous thromboembolism prophylaxis with low molecular weight heparin for 7 days.
Bibliography
- Neis, K. J., Zubke, W., Fehr, M., Römer, T., Tamussino, K., & Nothacker, M. (2016). Hysterectomy for Benign Uterine Disease. Deutsches Arzteblatt international, 113(14), 242–249. https://doi.org/10.3238/arztebl.2016.0242
- Sandberg, E. M., Hehenkamp, W., Geomini, P. M., Janssen, P. F., Jansen, F. W., & Twijnstra, A. (2017). Laparoscopic hysterectomy for benign indications: clinical practice guideline. Archives of gynecology and obstetrics, 296(3), 597–606. https://doi.org/10.1007/s00404-017-4467-9
- Encke, A., Haas, S., & Kopp, I. (2016). The Prophylaxis of Venous Thromboembolism. Deutsches Arzteblatt international, 113(31-32), 532–538. https://doi.org/10.3238/arztebl.2016.0532
