

Below we describe the laparoscopic modification by Trifyllis of the classic vaginal uterosacral ligament suspension.
Indication
- Uterine prolapse.
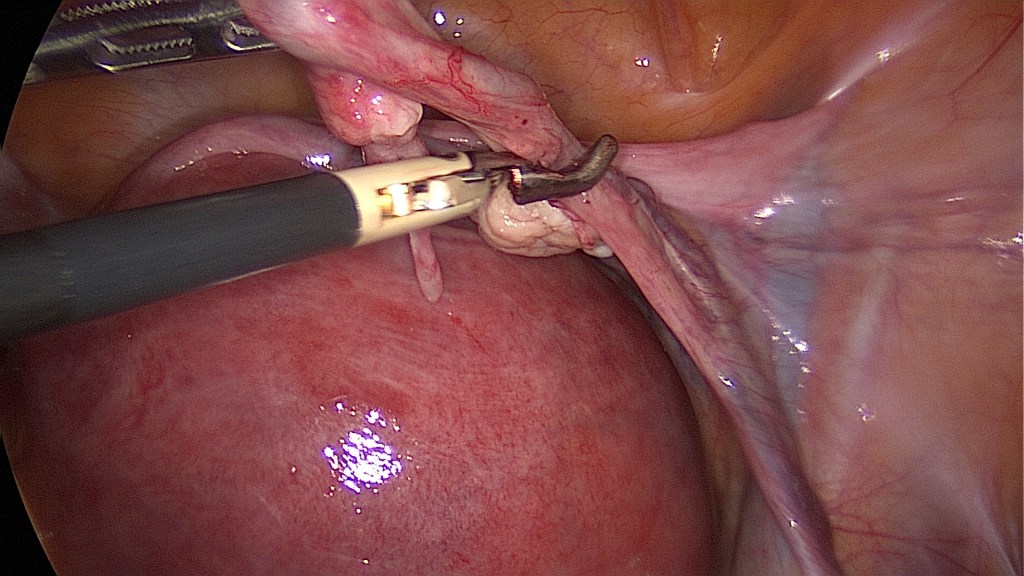
Prophylactic salpingectomy. 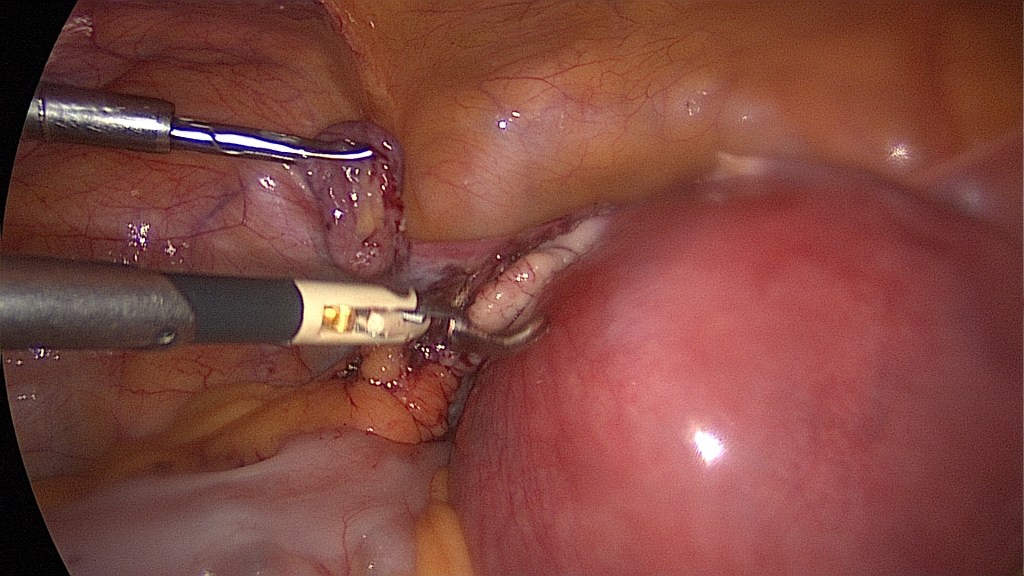
The removal of the fallopian tubes can be performed prior to the removal of the uterus, facilitating sight. 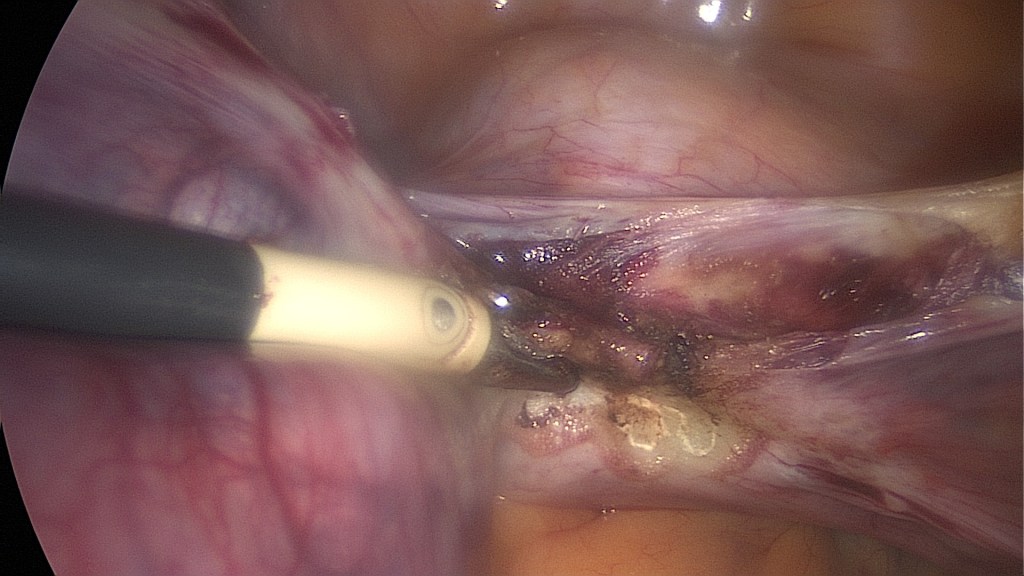
Coagulation of the uterine pedicle. 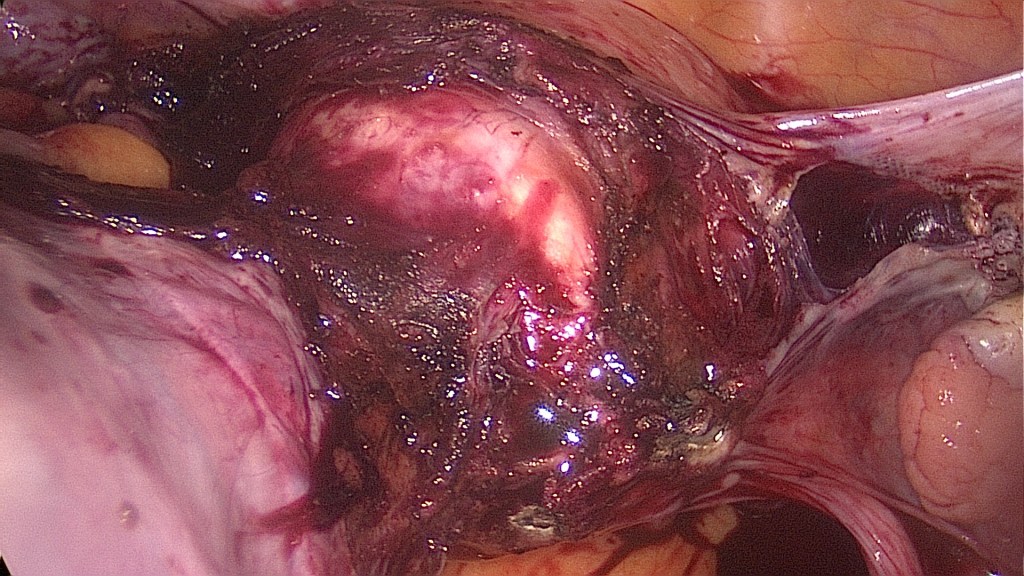
Dissection of the bladder and exposure of the vaginal wall. Caution is advised since injuries in the posterior side of the bladder can occur during vesicouterine dissection. 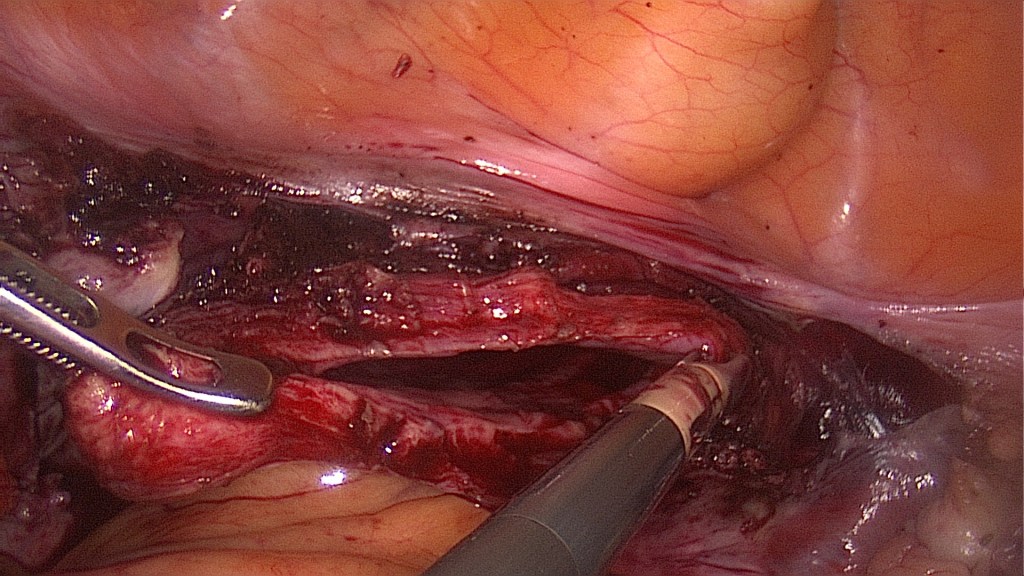
Site of the vaginal incision. 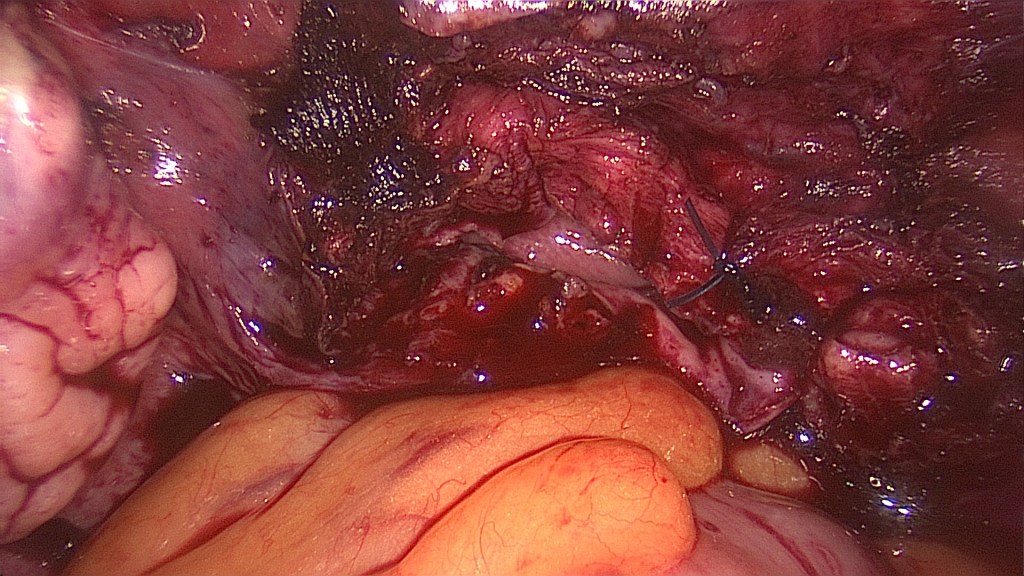
Passing of two figure of 8 sutures, one on each edge of the vaginal incision. Here the right one has been knotted. We prefer the extracorporeal knotting technique for the vaginal cuff. 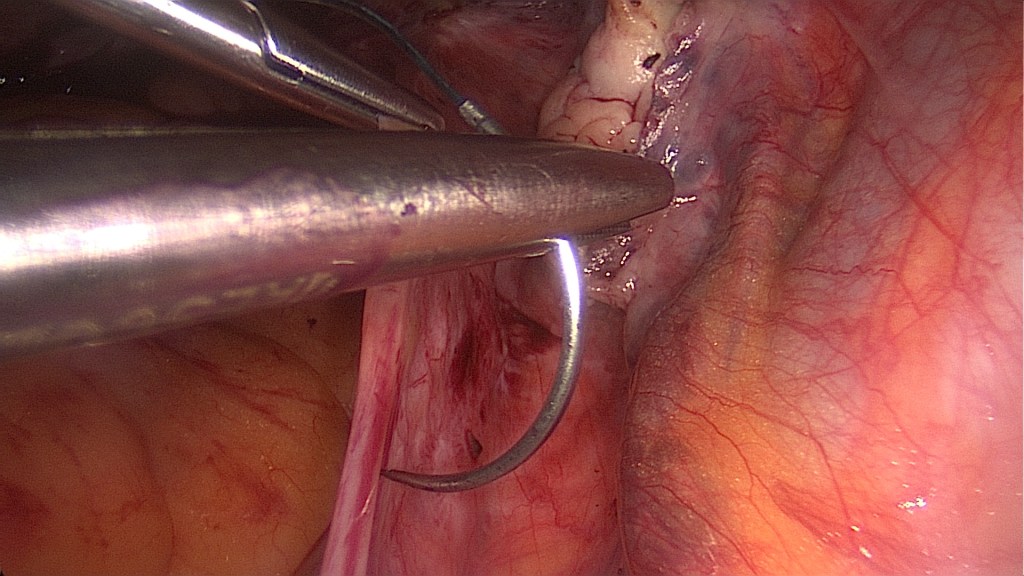
After the ureter has been identified, the right suspension suture is being placed as high as possible along the right uterosacral ligament (delayed absorbable 0 suture stitch). Preparation of the retroperitoneal space is not mandatory, but it may facilitate distancing the ipsilateral ureter and hypogastric nerve. 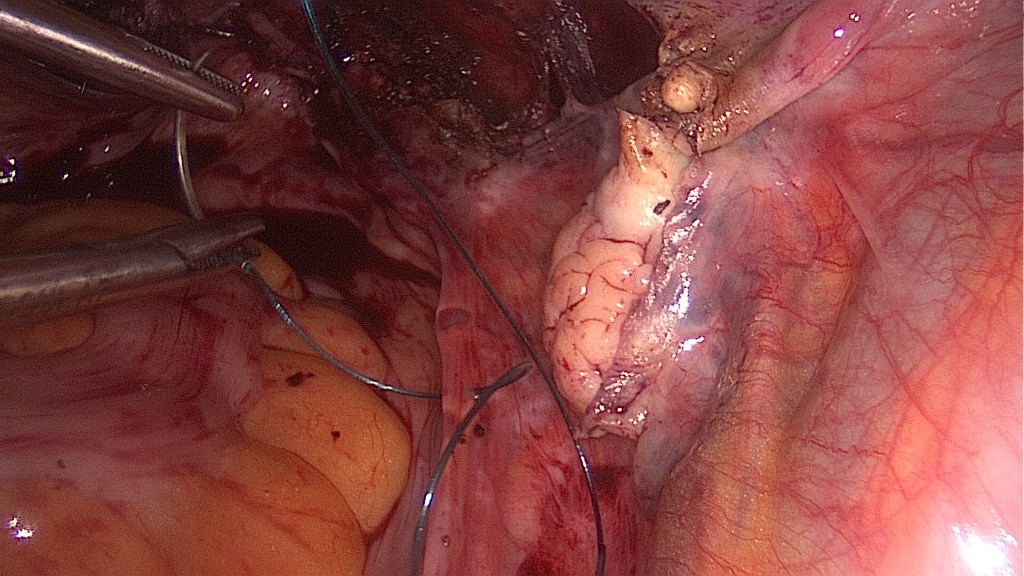
The suture passes a few times through the right uterosacral ligament for an efficient duplication. Respect the anatomy of the ureter, knowing that it approximates the uterosacral ligament the more caudally you get. 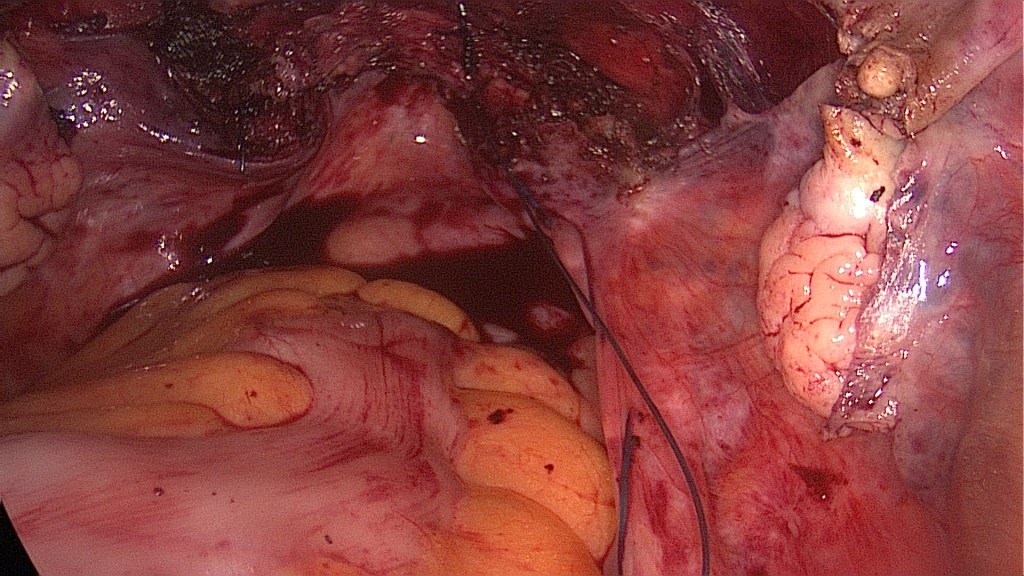
The suture is then passed through the posterior vaginal wall at the colpotomy site and both ends of the suture are being retrieved from the assistant on the vaginal side with a grasper under direct visualization. 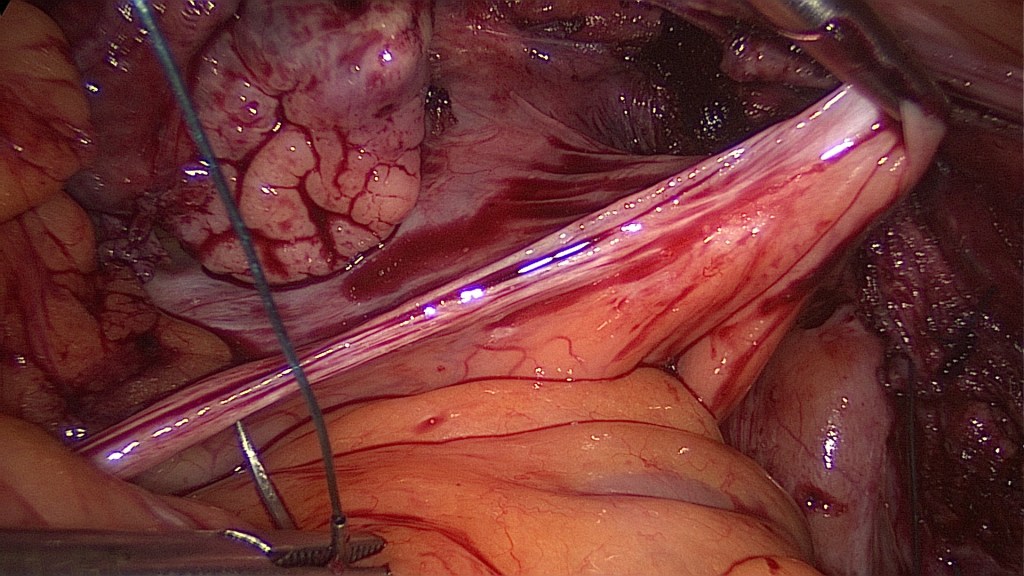
If the uterosacral ligament is not readily identified, gentle traction on its vaginal end is usually enough to demonstrate its path. 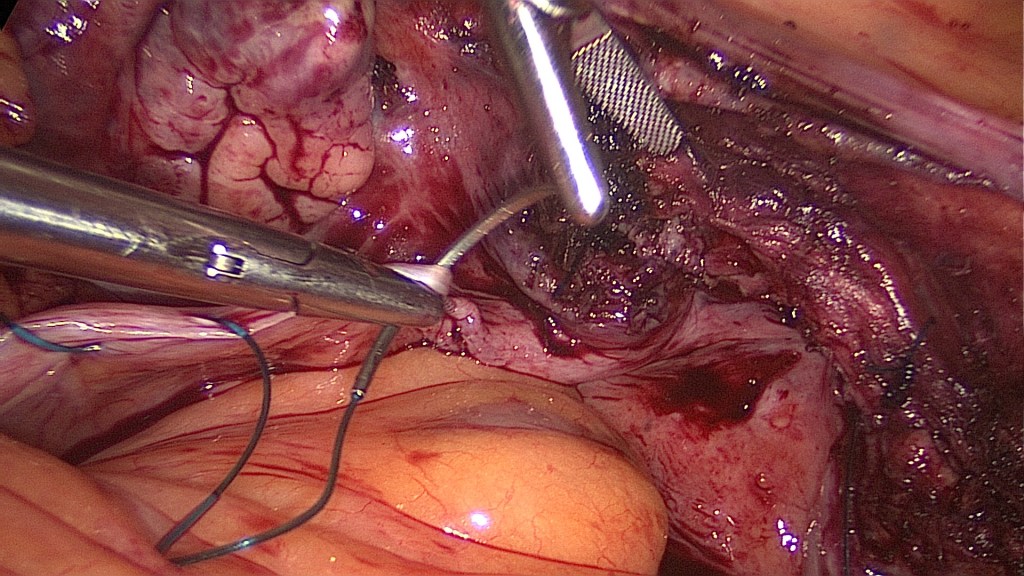
Duplication of the left uterosacral ligament. 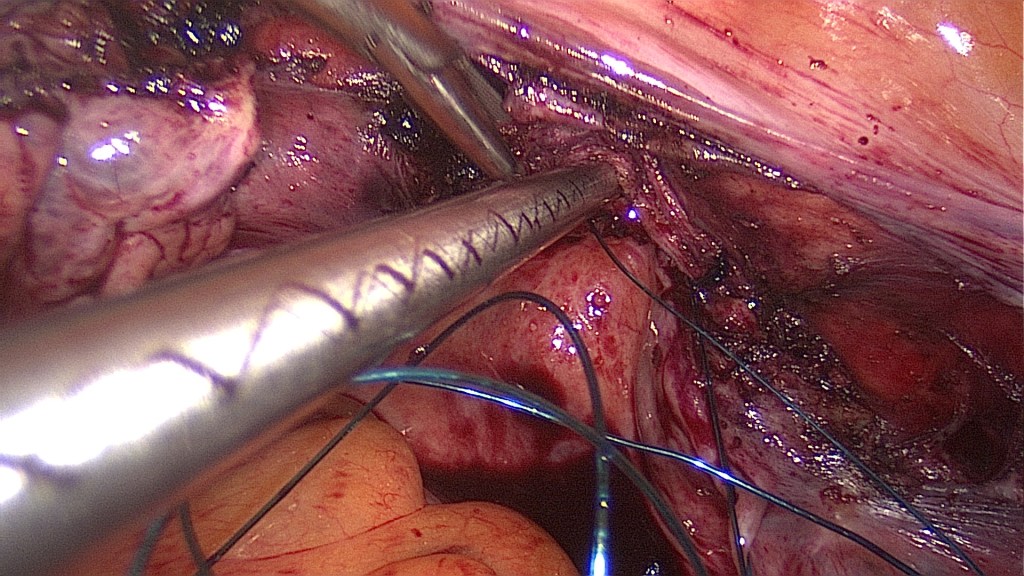
Extruding the thread towards the vagina. 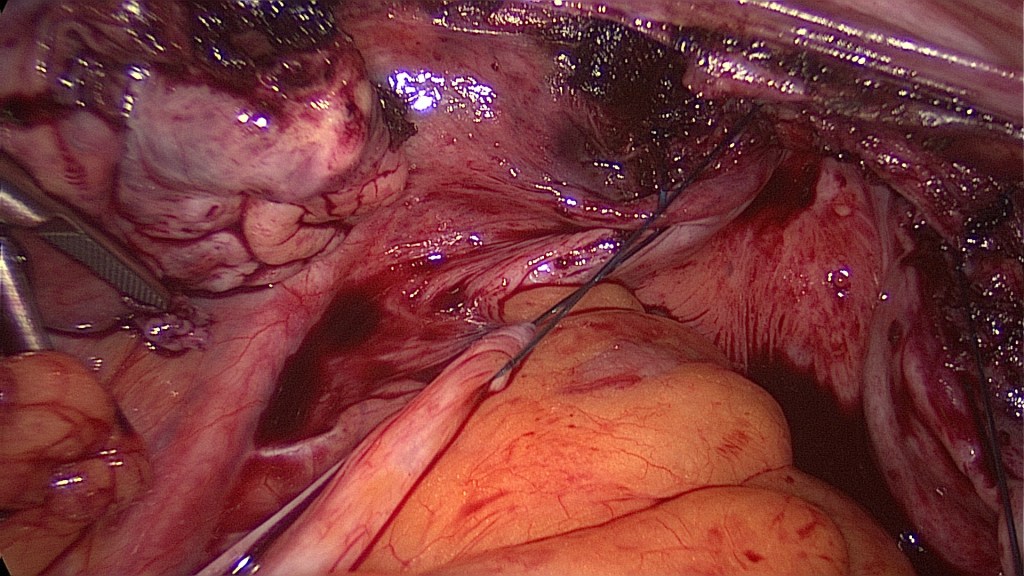
To avoid ureteral injury or kinking, ureteral peristalsis should be directly visualized. 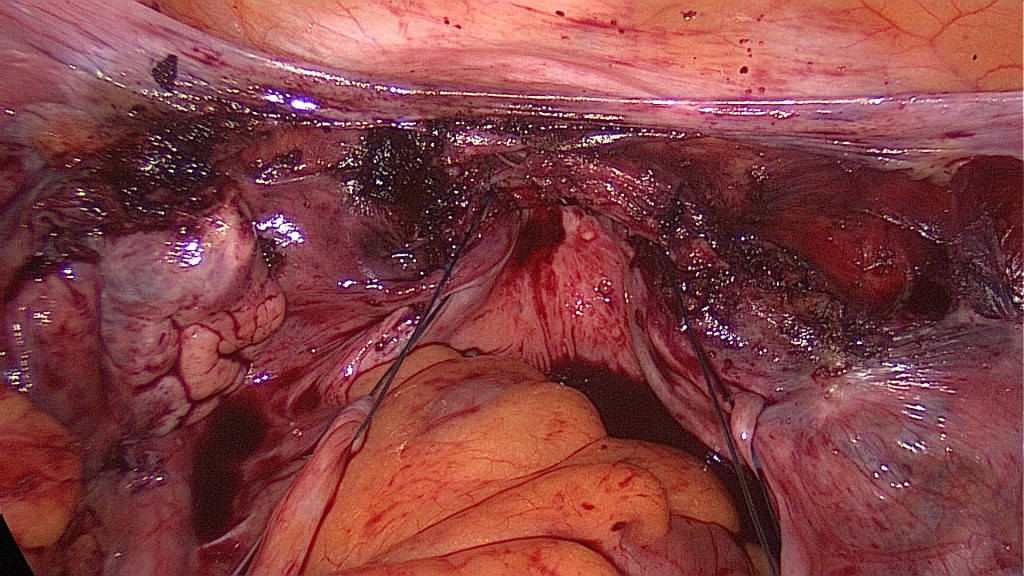
Image after placement of both suspension sutures. 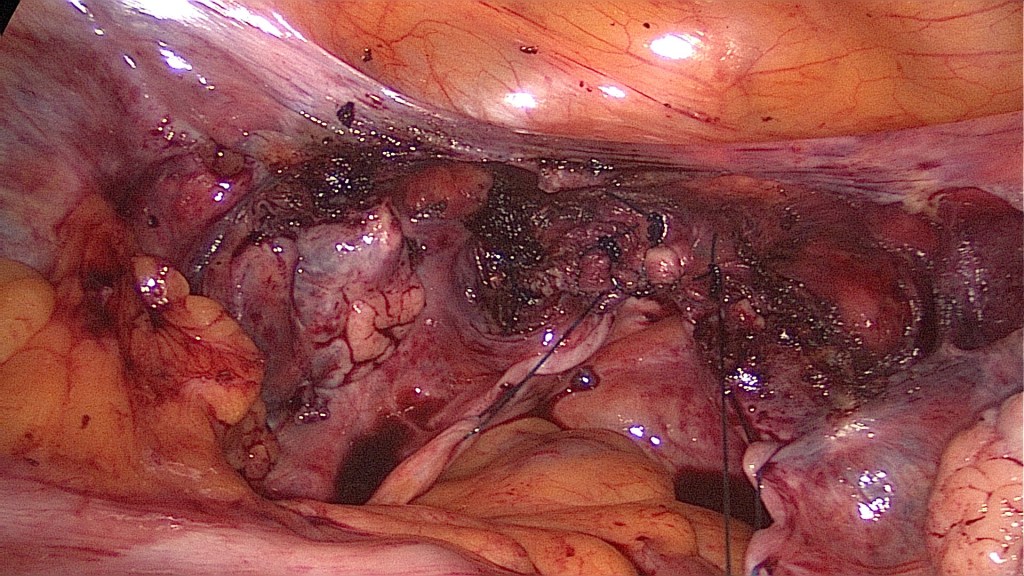
The vaginal cuff has been completely closed with four figure of 8 sutures. 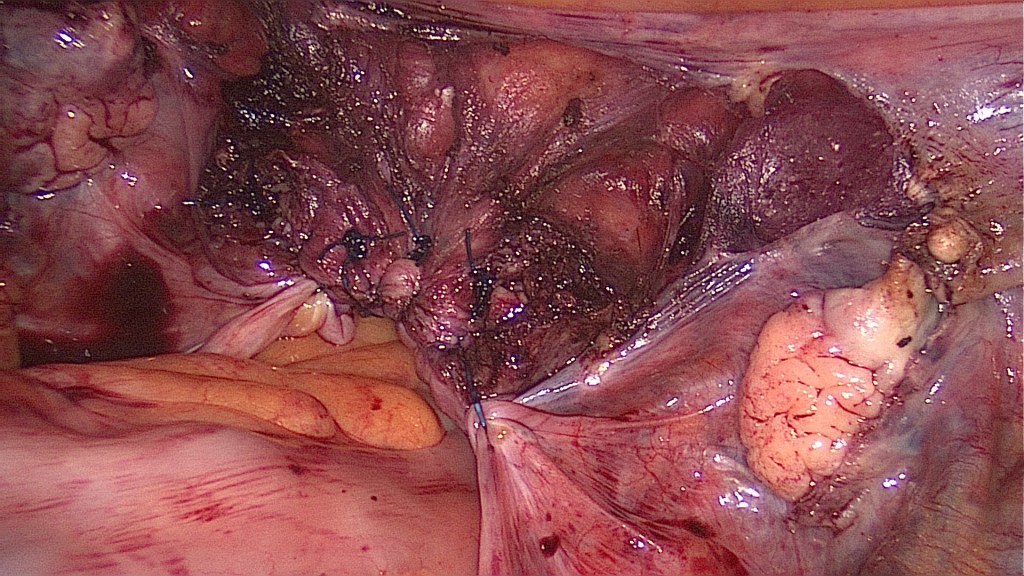
Image after tying the suspension knots vaginally.
Contraindications
- Obliteration of the pouch of Douglas.
Complications
- Ureteral injury or kinking and consequent hydronephrosis between 1.8% and 10.9% in international bibliography concerning the vaginal route. We estimate that this rate can be significantly lower with this laparoscopic technique.
- Prolapse recurrence.
Postoperative Management
- Nephrosonography for possible hydronephrosis. In case of hydronephrosis the ipsilateral suture has to be extracted.
Bibliography
- Aydin, C, Mercimek, MN. Laparoscopic management of bladder injury during total laparoscopic hysterectomy. Int J Clin Pract. 2020; 00:e13507. https://doi.org/10.1111/ijcp.13507
- Manodoro, S., Frigerio, M., Milani, R. et al. Tips and tricks for uterosacral ligament suspension: how to avoid ureteral injury. Int Urogynecol J 29, 161–163 (2018). https://doi.org/10.1007/s00192-017-3497-y
- Panico, G., Campagna, G., Caramazza, D. et al. Laparoscopic high uterosacral ligament suspension: an alternative route for a traditional technique. Int Urogynecol J 29, 1227–1229 (2018). https://doi.org/10.1007/s00192-018-3588-4
- Siff, Lauren N. MD; Jallad, Karl MD; Hickman, Lisa C. MD; Walters, Mark D. MD Surgical Anatomy of the Uterosacral Ligament Colpopexy, Female Pelvic Medicine & Reconstructive Surgery: September/October 2018 – Volume 24 – Issue 5 – p 380-382 doi: 10.1097/SPV.0000000000000461

2 Comments